Download
1 / 25
250 likes | 630 Views
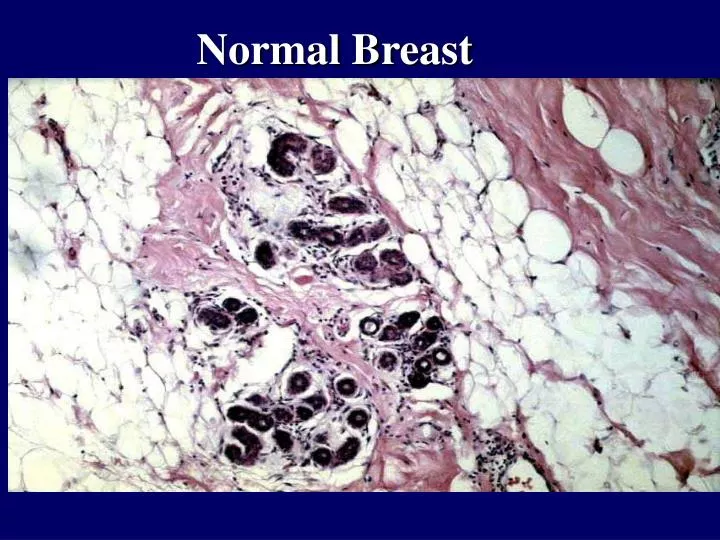
Normal Breast. Fibrocystic Change due to? Exaggeration of cyclic breast changes . Fibrocystic breast -- dilation of ducts produce microcysts and large cysts What distribution pattern? Multifocal and bilateral.

E N D
Fibrocystic Change due to? Exaggeration of cyclic breast changes
Fibrocystic breast -- dilation of ducts produce microcysts and large cysts What distribution pattern? Multifocal and bilateral
Sclerosing adenosis -- a proliferative fibrocystic change involving intralobular fibrosis and proliferation of small ductules and acini
There is prominent apocrine change of the cells lining the cysts in this example of fibrocystic changes of breast. Note the tall, pink, columnar nature of the epithelial cells. (Hey, it was mentioned in the slides and text, so here it is)
Ductal hyperplasia -- proliferative fibrocystic changes -- epithelia cells fill duct lumen which subtype has and increased risk for invasive carcinome? Atypical lobular hyperplasia
Fibroadenoma -- most common benign breast tumor -- most common ages? Puberty to 30 yoa -- fibrous stroma compressing glands, may grow during pregnancy
Intraductal papilloma -- in lactiferous duct --usually benign, solitary, but can recur - look for delicate papillomas in dilated duct What are symptoms? Serous, bloody discharge, nipple retraction
Ductal carcinoma in-situ -- Neoplastic cells are still within the ductules and have not broken through into the stroma. Note that the two large lobules in the center contain microcalcifications. Such microcalcifications can appear on mammography
Invasive ductal carcinoma with focal intraductal carcinoma, comedo-type (characterized by the presence of rapidly proliferating, high-grade malignant cells. Note the prominent central necrosis) ductal carcinomas make up about what % of breast carcinomas? 80%
This invasive ductal carcinoma of breast appears to radiate from a central area of desmoplasia. This collagenous component gives the neoplasm a hard "scirrhous" consistency that is palpable. Such an invasive carcinoma may be fixed to underlying chest wall, making it non-mobile.
Colloid carcinoma -- mucin extra and intracellularly -- soft masses
Medullary carcinoma -- lymph infiltrate -- tend to be large and softer
Tubular Carcinoma -- which three variants have better prognoses? Tubular, colloid, and medullary
Lobular carcinoma in situ -- terminal ducts and acini -- 9X risk for later lobular or ductal carc-- what population is lobular carc usually found? Young women
Infiltrating lobular carcinoma -- tend to be bilateral and multicentric -- tumor cells appear to be linearly arranged between stroma fibers
Infiltrating lobular carcinoma -- lines of cells Where are most carcinomas found and where do they mets? Outer upper quadrant to axillary lymph nodes
Paget’s Dz - (I put it in b/c it is in the text and other classes have discussed it) --large Paget's cells of Paget's disease of breast have abundant clear cytoplasm and appear in the epidermis either singly or in clusters. The nuclei of the Paget's cells are atypical and, though not seen here, often have prominent nucleoli. This dz often involves the nipple and areola. The dz starts as intraductal but extends to skin.