Download
1 / 22
220 likes | 489 Views
Endoluminal radiofrequency ablation and Endovenous laser therapy for the treatment of Varicose Veins: techniques and outcomes. Endoluminal radiofrequency ablation and Endovenous laser therapy for the treatment of Varicose Veins: techniques and outcomes.

E N D
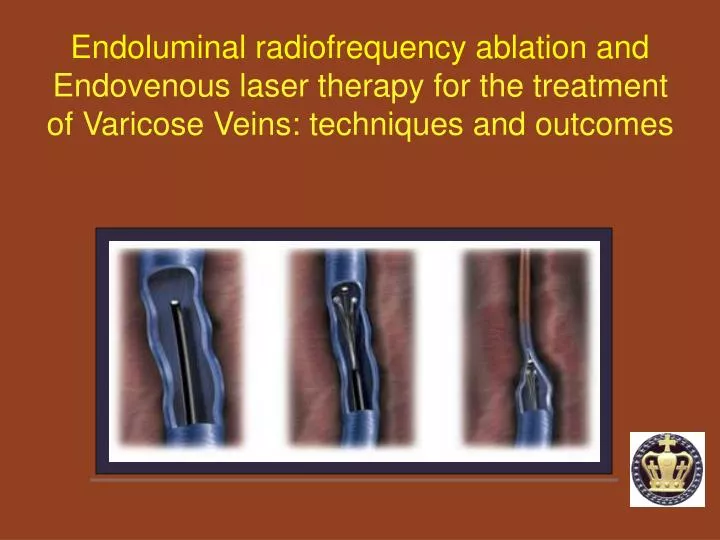
Endoluminal radiofrequency ablation and Endovenous laser therapy for the treatment of Varicose Veins: techniques and outcomes
Endoluminal radiofrequency ablation and Endovenous laser therapy for the treatment of Varicose Veins: techniques and outcomes • Clarify the indications for performing RFA and EVLT. • Explain the mechanisms, methods, of RFA and EVLT. • Outcomes of RFA and EVLT: response to treatment and • complications Bola Pratt P&S MS 4
Somewhere in Maui, Hawaii American Venous ForumFebruary of 1994 and the creation of CEAP klöf B, Rutherford RB, BerganJJ, Carpentier PH, Gloviczki P, Kistner RL, Meissner MH, Moneta GL, Myers K, Padberg FT, Perrin M, Ruckley CV, Smith PC, Wakefield TW; American Venous Forum International Ad Hoc Committee for Revision of the CEAP Classification. Revision of the CEAP classification for chronic venous disorders: consensus statement. J Vasc Surg. 2004 Dec;40(6):1248-52. Review. Bola Pratt P&S MS 4
Most Common Indications for EVLT or RFA: lessons from the American Venous ForumFebruary of 1994 and the creation of CEAP Clinical C0: No visible or palpable signs of venous disease C1: telangiectases or reticular veins C2: varicose veins C3: edema C4: skin changes ascribed to venous disease a. pigmentation or eczema b. lipodermatosclerosis or atrophie blanche C5: skin changes as defined previously with healed ulcer C6: skin changes as defined previously with active ulcer Etiologic: congenital, primary, secondary or noneAnatomic: superficial, perforator, deepor nonePathophysiologic: reflux, obstruction, both or none klöf B, Rutherford RB, BerganJJ, Carpentier PH, Gloviczki P, Kistner RL, Meissner MH, Moneta GL, Myers K, Padberg FT, Perrin M, Ruckley CV, Smith PC, Wakefield TW; American Venous Forum International Ad Hoc Committee for Revision of the CEAP Classification. Revision of the CEAP classification for chronic venous disorders: consensus statement. J Vasc Surg. 2004 Dec;40(6):1248-52. Review. Bola Pratt P&S MS 4
Endoluminal radiofrequency ablation (RFA) of the great saphenous vein: mechanism - By directing resistive radiofrequency energy through a vein, a narrow rim of tissue less than 1mm is heated by an electrode. - The amount of heating is modulated using both a microprocessor and manual movement, resulting in controlled collagen contraction, thermocoagulation and absorption of the vein. Puggioni A, Kalra M, Carmo M, Mozes G, Gloviczki P. Endovenous laser therapy and radiofrequency ablation of the great saphenous vein: analysis of early efficacy and complications.J Vasc Surg. 2005 Sep;42(3):488-93. Bola Pratt P&S MS 4
Endoluminal radiofrequency ablation of the great saphenous vein: methods Percutaneous access to the greater saphenous vein most commonly at the level of the knee under duplex ultrasound guidance Photograph courtesy of VNUS medical Technologies, San Jose, CA. Bola Pratt P&S MS 4
Endoluminal radiofrequency ablation of the great saphenous vein: methods 1) A guidewire is then advanced to the saphenofemoral junction over which the closure catheter is passed2) catheter prongs are extruded tocontact the intimal lining of the vessel wall3) radiofrequency generator allows the tip of the catheterand the prongs to attain a temperature of 85 degrees C. CFA = common femoral arteryCFV = common femoral veinSEV= superficial epigastric veinSFJ = saphenofemoral junction Photographs courtesy of VNUS medical Technologies, San Jose, CA. Bola Pratt P&S MS 4
Endoluminal radiofrequency ablation of the great saphenous vein: results 1) Vein occlusion at 1 week documented by venous ultrasound success rate of 98%2) None of the treated patients developed recanalization that was not seen at 6 weeks, with a successful outcome in 90%. 3) At the 24 month follow-up, 19 of 21 patients had complete disappearance of the treated saphenous vein, for a success rate of 90%. 4) Side effects were minimal, and no skin burns or thromboses were observed. Weiss RA, Weiss MA. Controlled radiofrequency endovenous occlusion using a unique radiofrequency catheter under duplex guidance to eliminate saphenous varicose vein reflux: a 2-year follow-up.Dermatol Surg. 2002 Jan;28(1):38-42. Bola Pratt P&S MS 4
Endovenous laser therapy (EVLT): mechanism - Thermal reaction after laser exposure is essential. - Damages endothelial, intimal internal elastic lamina, and to some degree the media. Adventitia is rarely affected. - In vitro studies suggest that energy results in ‘boiling of blood’ and and generation of ‘steam bubbles’ that indirectly, homogenously affect the varicose vein. Proebstle TM, Lehr HA, Kargl A, Espinola-Klein C, Rother W, Bethge S, Knop J. Endovenous treatment of the greater saphenous vein with a 940-nm diode laser: thrombotic occlusion after endoluminal thermal damage by laser-generated steam bubbles.J Vasc Surg. 2002 Apr;35(4):729-36. Bola Pratt P&S MS 4
Endovenous laser therapy: methods 1) GSV entered at the knee2) Guidewire passed through hollow needle into the vein can be difficult if: a. tortuosities b. local venous spasm c. sclerotic fragments3) Needle removed4) 3mm cutaneous incision made5) Introducer sheath placed over guide wire6) Guidewire removed when at the SFJ7) Longitudinal US visualization of sheath 1-2 cm distally to the SFJ van den Bos RR, Kockaert MA, Neumann HA, Nijsten T.Technical review of endovenous laser therapy for varicose veins. Eur J Vasc Endovasc Surg. 2008 Jan;35(1):88-95. Epub 2007 Oct 24. Review. Bola Pratt P&S MS 4
Endovenous laser therapy and radiofrequency: methods Tumescent anesthesia (5 ml epi, 5 ml bicarb, 35ml 1% lidocaine in 500ml saline) is administered to the perivenous space resulting ina) reduction in painb) protection of perivenous tissue through coolingc) increase in surface area of laser tip and vein wall van den Bos RR, Kockaert MA, Neumann HA, Nijsten T.Technical review of endovenous laser therapy for varicose veins. Eur J Vasc Endovasc Surg. 2008 Jan;35(1):88-95. Epub 2007 Oct 24. Review. Bola Pratt P&S MS 4
Endovenous laser therapy and radiofrequency: specifics Pulsed vs. continuous: pulsed mode is associated with higher adverse eventsWavelengths: Higher wavelengths (1320nm) reported less postoperative pain, and less likely to have ecchymosesFluence (J/ cm2): Single most important parameter to quantify above 60-100 J/ cm2 for durable GSV occlusionWattage: high, short duration wattage vaporizing effect low prolonged wattage coagulating effectPullback Speed: if performed at fixed wattage then energy is solely dependent on pullback speed Bola Pratt P&S MS 4
Endovenous laser therapy and radiofrequency: results Pretreatment: an incompetent SFJ Posttreatment: occlusion of GSV Puggioni A, Kalra M, Carmo M, Mozes G, Gloviczki P. Endovenous laser therapy and radiofrequency ablation of the great saphenous vein: analysis of early efficacy and complications. J Vasc Surg. 2005 Sep;42(3):488-93. Bola Pratt P&S MS 4
Endovenous laser therapy and radiofrequency: results van den Bos RR, Kockaert MA, Neumann HA, Nijsten T.Technical review of endovenous laser therapy for varicose veins. Eur J Vasc Endovasc Surg. 2008 Jan;35(1):88-95. Epub 2007 Oct 24. Review. Bola Pratt P&S MS 4
Burden of repeated treatment and complications ? EVLT vs. RFA of the great saphenous vein: outcomes, complications EVLT RFA Bola Pratt P&S MS 4
Most Common Indications for EVLT or RFA: lessons from the American Venous ForumFebruary of 1994 and the creation of CEAP Clinical C0: No visible or palpable signs of venous disease C1: telangiectases or reticular veins C2: varicose veins C3: edema C4: skin changes ascribed to venous disease a. pigmentation or eczema b. lipodermatosclerosis or atrophie blanche C5: skin changes as defined previously with healed ulcer C6: skin changes as defined previously with active ulcer Etiologic: congenital, primary, secondary or noneAnatomic: superficial, perforator, deepor nonePathophysiologic: reflux, obstruction, both or none klöf B, Rutherford RB, BerganJJ, Carpentier PH, Gloviczki P, Kistner RL, Meissner MH, Moneta GL, Myers K, Padberg FT, Perrin M, Ruckley CV, Smith PC, Wakefield TW; American Venous Forum International Ad Hoc Committee for Revision of the CEAP Classification. Revision of the CEAP classification for chronic venous disorders: consensus statement. J Vasc Surg. 2004 Dec;40(6):1248-52. Review. Bola Pratt P&S MS 4
Puggioni et al 2005: Retrospective review of 92 patients, 130 limbs All had: symptomatic varicose veins by CEAP criteriaWomenClinical Presentation: C2-4Etiology: primary EVLT RFA Veins of all sizes: 14 W; 810nm; 3mm/s withdrawing speed Veins 2 - 12mm: Temp 82- 90; 3cm/min withdrawing speed Puggioni A, Kalra M, Carmo M, Mozes G, Gloviczki P. Endovenous laser therapy and radiofrequency ablation of the great saphenous vein: analysis of early efficacy and complications. J Vasc Surg. 2005 Sep;42(3):488-93. Bola Pratt P&S MS 4
EVLT and RFA analysis of early complications: Puggioni et al 2005 Puggioni A, Kalra M, Carmo M, Mozes G, Gloviczki P. Endovenous laser therapy and radiofrequency ablation of the great saphenous vein: analysis of early efficacy and complications.J Vasc Surg. 2005 Sep;42(3):488-93. Bola Pratt P&S MS 4
Puggioni et al 2005 conclusion • EVLT was associated with a somewhat higher occlusion rate, but post-op complications were more frequent- All patients should undergo early post-operative duplex to rule out proximal extension of thrombus, exclude distal DVT, and confirm occlusion Puggioni A, Kalra M, Carmo M, Mozes G, Gloviczki P. Endovenous laser therapy and radiofrequency ablation of the great saphenous vein: analysis of early efficacy and complications.J Vasc Surg. 2005 Sep;42(3):488-93. Bola Pratt P&S MS 4
RFA and DVT analysis: Hingorani et al 2004 • DVT in 12 limbs (16%)- no difference in DVT between men and women- catheter size: no difference in DVT - anesthesia: no difference in DVT - higher incidence of DVT with RFA and vein excision Hingorani AP, Ascher E, Markevich N, Schutzer RW, Kallakuri S, Hou A, Nahata S, Yorkovich W, Jacob T. Deep venous thrombosis after radiofrequency ablation of greater saphenous vein: a word of caution.J Vasc Surg. 2004 Sep;40(3):500-4.
Summary • EVLT and RFA are associated with a high degree of success with minimal side effects most of which can be prevented or minimized with minor modifications of technique.- All patients should undergo early post-operative duplex to rule out proximal extension of thrombus, exclude distal DVT, and confirm occlusion.- The advantage EVLT has over RFA is the lower cost per patient and possibly faster treatment than RF closure. P&S
References klöf B, Rutherford RB, BerganJJ, Carpentier PH, Gloviczki P, Kistner RL, Meissner MH, Moneta GL, Myers K, Padberg FT, Perrin M, Ruckley CV, Smith PC, Wakefield TW; American Venous Forum International Ad Hoc Committee for Revision of the CEAP Classification. Revision of the CEAP classification for chronic venous disorders: consensus statement. J Vasc Surg. 2004 Dec;40(6):1248-52. Review. Proebstle TM, Lehr HA, Kargl A, Espinola-Klein C, Rother W, Bethge S, Knop J. Endovenous treatment of the greater saphenous vein with a 940-nm diode laser: thrombotic occlusion after endoluminal thermal damage by laser-generated steam bubbles.J Vasc Surg. 2002 Apr;35(4):729-36. Puggioni A, Kalra M, Carmo M, Mozes G, Gloviczki P. Endovenous laser therapy and radiofrequency ablation of the great saphenous vein: analysis of early efficacy and complications.J Vasc Surg. 2005 Sep;42(3):488-93. van den Bos RR, Kockaert MA, Neumann HA, Nijsten T.Technical review of endovenous laser therapy for varicose veins. Eur J Vasc Endovasc Surg. 2008 Jan;35(1):88-95. Epub 2007 Oct 24. Review. Weiss RA, Weiss MA. Controlled radiofrequency endovenous occlusion using a unique radiofrequency catheter under duplex guidance to eliminate saphenous varicose vein reflux: a 2-year follow-up.Dermatol Surg. 2002 Jan;28(1):38-42. P&S