Download
1 / 1
10 likes | 107 Views
In-hospital hospice units: a novel approach to care in the final days. Introduction:

E N D
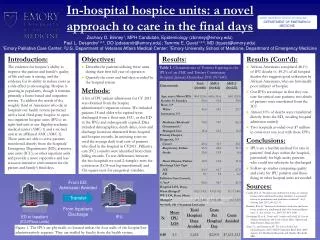
In-hospital hospice units: a novel approach to care in the final days Introduction: The evidence for hospice’s ability to improve the patient and family’s quality of life and care is strong, and the evidence for its ability to reduce costs as a side effect is encouraging. Hospice is growing in popularity, though it remains primarily a home-based and outpatient service. To address the needs of the roughly third of Americans who die in hospitals our health system partnered with a local third-party hospice to open two inpatient hospice units (IPUs): an eight-bed unit at our flagship academic medical center (AMC-1) and a six-bed unit at an affiliated AMC (AMC-2). These units are able to serve patients transferred directly from the hospitals’ Emergency Departments (ED), intensive care units (ICU), or other inpatient units and provide a more supportive and less resource-intensive environment for the patient and family’s final days. Objectives: Describe the patients utilizing these units during their first full year of operation Quantify the costs and bed-days avoided by the hospital system Methods: A list of IPU patient admissions for CY 2011 was obtained from the hospice administrator’s inpatient census. We included patients 18 and older who expired were discharged from a floor unit, ICU, or the ED to the IPUs and subsequently expired. Data included demographics, death dates, costs and discharge locations abstracted from hospital and hospice records. In assessing costs we used the average daily total cost of patients who died in the hospital in CY2011. Palliative care (PC) consults were identified from clinic billing records. To test differences between the two hospitals we used 2-sample t-tests for continuous (LOS was log-transformed) and Chi-square tests for categorical variables. Results (Cont’d): African-Americans comprised 48.1% of IPU deaths vs. 49.2% of all hospital deaths; this suggests good utilization by African-Americans, who are historically poor utilizers of hospice Our IPUs are unique in that they can care for critical care patients; two-thirds of patients were transferred from the ICU Almost 10% of deaths were transferred directly from the ED, avoiding hospital admission entirely Two hospitals avoided over $7 million in costs over one year with these IPUs Conclusions: IPUs are a feasible method for care in patients’ final days within the hospital, particularly for high-acuity patients who could not otherwise be discharged Follow-up studies comparing quality and costs for IPU patients and those dying in other hospital units are needed Sources: Candy, B et al. “Hospice care delivered at home, in nursing homes and in dedicated hospice facilities: A systematic review of quantitative and qualitative evidence.” Int J Nursing Stud. 2011; 48: 121-33. Brumley R et al. “Increased satisfaction with care and lower costs: results of a randomized trial of in-home palliative care.” J. Am. Geriatr. Soc., 2007; 55: 993–1000. Goodman, D et al. Trends and Variation in End-of-Life Care for Medicare Beneficiaries with Severe Chronic Illness. Dartmouth Atlas Project, Hanover, NH. Zhao, Y., and Encinosa, W. The Cost of End-of-Life Hospitalizations, 2007. HCUP Statistical Brief #81. 2009. Agency for Healthcare Research and Quality, Rockville, MD. Results: EMORY UNIVERSITY SCHOOL OF MEDICINE DEPARTMENT OF EMERGENCY MEDICINE Zachary O. Binney1, MPH Candidate, Epidemiology (zbinney@emory.edu) Paul L. Desandre1,2,3, DO (pdesandr@emory.edu); Tammie E. Quest1,2,3, MD (tquest@emory.edu)1Emory Palliative Care Center; 2U.S. Department of Veterans Affairs Medical Center; 3Emory University School of Medicine, Department of Emergency Medicine Table 1. Characteristics of Patients Expiring in the IPUs of an AMC and Tertiary Community Hospital, January-December 2011 (N=640). From ED: Admission Avoided Transfer Table 2. Cost Impact for Hospitals of Patients Successfully Transferred to IPU (N=640). From Inpatient: Discharge ED or Inpatient (ICU/Floor units) IPU Figure 1. The IPUs are physically co-located within the four walls of the hospital but administratively separate. They are staffed by faculty from the health system.