Download

1 / 171
1.72k likes | 1.75k Views
Explore treatment options for hypertension in diabetes patients and atrial fibrillation, essential hypertension management, metabolic syndrome criteria, EKG abnormalities, and hypertension causes in different age groups.

E N D
1. A 65-year-old male comes to your office for an initial visit. He has a 5 year history of type 2 diabetes treated with glipizide (Glucotrol), 10 mg/d. A physical examination is notable for a blood pressure of 142/92 mm Hg and nonproliferative diabetic retinopathy with scattered microaneurysms and cotton-wool spots. On laboratory evaluation he is found to have a glycosylated hemoglobin of 8.4%, a serum creatinine level of 1.3 mg/dL, and microalbuminuria. You consider prescribing an antihypertensive agent. Agents which have been shown to slow the progression of microalbuminuria to macroalbuminuria in this situation, independent of blood pressure reduction, include which of the following? • ACE inhibitors • Dihydropyridine calcium channel blockers • Angiotensin receptor blockers • Hydrochlorothiazide • ß-Blockers
Microalbuminuria • Important prognostic marker for kidney dz • 30-300 mg/L on spot microalbumin urine check (2 measures over 2-3 month period) • Albumin/Creatinine Ratio: > 3.5 in females > 2.5 in males
Delaying Progression to Macroalbuminuria • ACE Inhibitors • Angiotensin Receptor Blockers (ARBs)
2. In a hypertensive patient with atrial fibrillation, which of the following antihypertensive agents will also help control the ventricular rate? (Mark all that are true.) • Metoprolol (Lopressor) • Verapamil (Calan, Isoptin) • Amlodipine (Norvasc) • Diltiazem (Cardizem) • Nifedipine (Adalat, Procardia)
Normal Conduction Pathway Atrial Fibrillation
Slowing Sinus and AV Node Conduction • Beta-blockers • Non-dihydropyridine Calcium Channel Blockers • Verapamil • Diltiazem
3. A 16-year-old sexually active female is diagnosed with essential hypertension. Despite a 6-month trial of lifestyle modification, her blood pressure continues to be in the range of 150/98 mm Hg. Which of the following should be avoided in this patient? (Mark all that are true.) • Thiazide diuretics • ACE inhibitors • Angiotensin II antagonists • ß-Blockers • Calcium channel blockers
Avoid in Pregnancy • ACE-Inhibitors • ARBs • Risk of Fetal Developmental Abnormalities • Cardiovascular malformations • CNS malformations • Fetal and Neonatal Problems (2-3 trimester) • Hypotension, skull hypoplasia, anuria, renal failure, death
4. According to National Cholesterol Education Program guidelines, criteria for the diagnosis of metabolic syndrome include which of the following? (Mark all that are true.) • A waist circumference >40 inches in a male • An HDL-cholesterol level ≤ 50 mg/dL in women • An LDL-cholesterol level > 160 mg/dL • Serum triglycerides ≥ 150 mg/dL • Blood pressure ≥ 130 mm Hg systolic and/or 85 mm diastolic
Metabolic Syndrome • Constellation of CV Risk Factors related to: • Hypertension • Abdominal Obesity • Dyslipidemia • Insulin Resistance
Metabolic Syndrome • National Cholesterol Education Program (NCEP) Diagnostic Criteria (> 3): • Obesity (Waist Circumference) • 40 inches in Men • 35 inches in Women • BP > 130 mm Hg Systolic and/or 85 mm Diastolic • Fasting Glucose > 110 • Triglycerides > 150 mg/dL • HDL Cholesterol • < 40 mg/dL Men • < 50 mg/dL Women
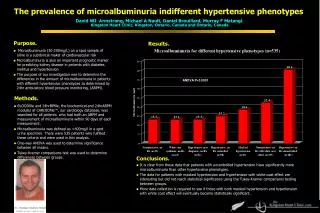
5. You see a 65-year-old African-American female for her annual physical examination. Her past medical history is notable for a 15-year history of hypertension and a 10-year history of type 2 diabetes mellitus. To assess for possible end-organ effects of her hypertension and diabetes, you order an EKG, which is shown below. Abnormalities shown on the EKG include which of the following? (Mark all that are true.) • Left ventricular hypertrophy • Left bundle-branch block • Anteroseptal infarct, age undetermined • Inferior infarct, age determined • Lateral wall infarct, age undetermined
3 Points ST forces in direction opposite to R wave in lateral chest leads Largest R or S wave in limb lead is 20 mm or more OR the largest S wave V1, V2, or V3 is 25 mm or more P-terminal force in in V1 is 0.04 or more 2 Points Left axis deviation greater than -15 degree 1 Point QRS duration > 0.09 Intrinsicoid deflection in V5-V6 is 0.04 seconds or later > 5 = LVH 4 = Probable LVH Estes Criteria for LVH
6. A 39-year-old white male sees you for evaluation of high blood pressure. His past medical history is unremarkable. Examination reveals an obese male with a round face and plethoric complexion. His blood pressure is 150/98 mm Hg, pulse 88 beats/min, and respiratory rate 16/min. Other notable findings include a prominent dorsal cervical fat pad and supraclavicular fat pads, as well as violaceous striae on his trunk. A laboratory evaluation is notable only for a fasting glucose level of 114 mg/dL. What is the most likely cause of his hypertension?
Hyperadrenalcorticalismi.e.: Cushing’s Syndrome Emotional disturbance Enlarged sella turcica Moon facies Osteoporosis Cardiac Hypertrophy (hypertension Buffalo Hump Obesity Adrenal tumor or hyperplasia Thin, wrinkled skin Abdominal striae Amenorrhea Muscle Weakness Purpura Poor Wound Healing Glucose intolerance
7. Risk factors for acute renal failure induced by ACE inhibitors and angiotensin receptor blockers include which of the following? (Mark all that are true.) • Reduced arterial blood volume • Renal artery stenosis • Polycystic kidney disease • Use of cyclosporine (Sandimmune) • Use of NSAIDs
ACE Inhibitor ARB
Risk Factors for Acute Renal Failure • Reduced arterial blood volume • Absolute or effective • Renal artery stenosis • Polycystic kidney disease • Use of cyclosporine (Sandimmune) or tacrolimus • Use of NSAIDs • Sepsis
8. Antihypertensive agents likely to be effective as monotherapy in African-Americans include which of the following? (Mark all that are true.) • Thiazide diuretics • ACE inhibitors • Angiotensin II antagonists • ß-Blockers • Long-acting dihydropyridine calcium channel blockers
Source: Centers for Disease Control and National Center for Health Statistics, National Health Interview Survey and National Hospital Discharge Survey
Monotherapy in African Americans • Long-acting calcium channel blockers • Diuretics
9. An agent other than a thiazide diuretic should be considered for initial antihypertensive therapy in patients with which of the following? (Mark all that are true.) • Gout • Diabetes mellitus • Bipolar disorder treated with lithium • Chronic renal insufficiency, with a serum creatinine level of 2.6 mg/dL • A past history of stroke
Thiazide Contraindications • Renal Insufficiency • Ineffective • Gout • May increase serum uric acid • Lithium Therapy • Enhance renal tubular absorbtion
Mark all options that are consistent with the recommendations of JNC-7. • Systolic blood pressure is classified as normal if it is below 120 mm Hg • Diastolic blood pressure is classified as normal if it is below 80 mm Hg • Prehypertension is defined as a systolic blood pressure of 130–139 mm Hg and/or a diastolic blood pressure of 85–89 mm Hg • Stage 2 hypertension is defined as a systolic blood pressure ≥ 160 mm Hg and/or a diastolic blood pressure ≥ 100 mm Hg • If a patient's systolic and diastolic readings fall into different categories, the lowest of the two categories determines the patient's blood pressure classification
JNC-7 Classification of Blood Pressure Stage 2 Hypertension Stage 1 Hypertension Prehypertension (or) Normal (and)
11. A patient with bipolar disorder which is well-controlled by lithium is diagnosed with essential hypertension. Which of the following antihypertensive agents should be avoided because they can raise serum lithium levels? (Mark all that are true.) • Thiazide diuretics • -Blockers • Direct vasodilators • ACE inhibitors • 1-Blockers
Lithium and Hypertension • Diuretics • Decrease renal clearance • ACE inhibitors • Increase steady-state plasma levels
12. Mark all options that are true regarding home blood pressure monitoring. • It can foster patient adherence • It may be useful for assessing white coat hypertension • A home blood pressure reading of 130/80 mm Hg is regarded as comparable to 140/90 mm Hg measured in the office • Wrist blood pressure devices are as accurate as arm-cuff devices • Home blood pressure devices should be regularly checked against the family physician's office blood pressure unit
Ambulatory Blood Pressure Monitoring • Improves adherence to therapy • Provides information about “White Coat” hypertension • > 135/85 at home = HTN (140/90) • Calibrate regularly with clinic device • Only properly sized arm cuffs should be used
13. A 65-year-old African-American male with a history of coronary heart disease and heart failure (left ventricular ejection fraction 38%) is diagnosed with hypertension. Which of the following blood pressure medications should be AVOIDED? (Mark all that are true.) • Diltiazem (Cardizem) • Moxonidine (NOT AVAILABLE IN U.S.) • Metoprolol (Lopressor, Toprol) • Doxazosin (Cardura) • Hydralazine
Medications to avoid in CHF with HTN • Nondihydropyridine CCB’s • Diltiazem and Verapamil • Moxonidine and Clonidine • Alpha-blockers • Doxazosin
14. Isolated systolic hypertension in a young child suggests which of the following diagnoses? (Mark all that are true.) • Coarctation of the aorta • Renovascular hypertension due to fibromuscular dysplasia C. Pheochromocytoma D. Patent ductus arteriosus E. Hyperthyroidism
Isolated Systolic HTN in Children • Coarctation of the Aorta • Patent ductus arteriosus • Hyperthyroidism
15. True statements regarding the effect of aerobic exercise on blood pressure include which of the following? (Mark all that are true.) • Aerobic exercise reduces blood pressure in both hypertensive and normotensive patients • Aerobic exercise has been shown to lower systolic blood pressure by 4–9 mm Hg • Aerobic exercise has been shown to reduce insulin resistance in hypertensive patients • The beneficial impact of aerobic exercise on blood pressure is dependent on weight loss • Sedentary individuals have a 30%–50% higher risk of developing hypertension compared to those who exercise regularly
Aerobic Exercise and Blood Pressure • Reduces BP in HTN and normotensive • Reduces insulin resistance • 4-9 mm decrease in SBP • Independent of weight loss • Sedentary 20-50% increased risk for HTN
Guidelines for healthy adults under age 65 Basic recommendations from ACSM and AHA: Do moderately intense cardio 30 minutes a day, five days a weekOrDo vigorously intense cardio 20 minutes a day, 3 days a weekAndDo eight to 10 strength-training exercises, eight to 12 repetitions of each exercise twice a week.
16. A 62-year-old homeless male has a long history of hypertension treated with clonidine (Catapres), 0.6 mg twice a day. You see him at the clinic at the homeless shelter, and he tells you that he ran out of his medication 2 days ago. He reports no complaints other than feeling “sort of on edge.” A physical examination is notable only for a blood pressure of 170/105 mm Hg. Which of the following classes of antihypertensive agents can increase the severity of his rebound hypertension? (Mark all that are true.) • Thiazide diuretics • ACE inhibitors • Angiotensin II antagonists • ß-Blockers • Long-acting dihydropyridine calcium channel blockers
16 Rebound from Antihypertensives • The sudden cessation of clonidine, a centrally-acting alpha-2-agonist, can result in an abrupt rise in hypertension - a result of a rebound phenomenon causing sympathetic overactivity. • In this state of increased levels of catecholamines, beta-blockers will neutralize the vasodilatory effects of peripheral vascular beta-receptors. • Effectively leaves the vasoconstrictor alpha-receptors unopposed and can result in a further rise in blood pressure.
17. Antihypertensive agents associated with increases in serum triglycerides include which of the following? (Mark all that are true.) • Thiazide diuretics • ACE inhibitors • Angiotensin II antagonists • ß-Blockers • Long-acting dihydropyridine calcium channel blockers
Cyclosporine Protease Inhibitors Diuretics Estrogens Prednisone Amiodarone Progestins Anabolic steroids Medicines that cause Hypertriglyceridemia 17
Diuretics and TG • Thiazide diuretics cause a temporary increase in TC levels, TG, and LDL. • Increase may range between 5 to 10 milligrams per deciliter. • Indapamide is the only thiazide diuretic that has not been shown to raise cholesterol levels. • Loop diuretics share same pattern as THZ; occ. also see a decrease in HDL.
18. A 22-year-old secretary is referred to you for evaluation of high blood pressure. Her past medical history is unremarkable and she is on no prescriptions or over-the-counter medications. Her review of systems reveals only a chronic history of mild fatigue and episodic muscle cramping. Her physical examination is normal except for a blood pressure of 156/100 mm Hg in both arms without significant orthostatic changes. Laboratory Findings CBC.................................... Normal Urinalysis................................ Normal Serum sodium. .............. 145 mmol/L (N 135–145) Serum potassium. ............. 2.9 mmol/L (N 3.5–5.0) Serum chloride............... 100 mmol/L (N 100–108) Serum bicarbonate. .............. 25 mmol/L (N22–26) Serum creatinine................ 0.7 mg/dL (N 0.6–1.5) BUN........................... 10 mg/dL (N 8–25) Serum glucose.......................... 90 mg/dL What is the most likely cause of her hypertension?
18 Primary Aldosteronism • Overproduction of aldosterone • Due to adrenal hyperplasia, CA, or adrenal adenoma • Twice as common in women as in men • Usually occurs between 30 and 50 y/o. • 1% of unselected hypertensive patients.