Download
1 / 1
10 likes | 145 Views
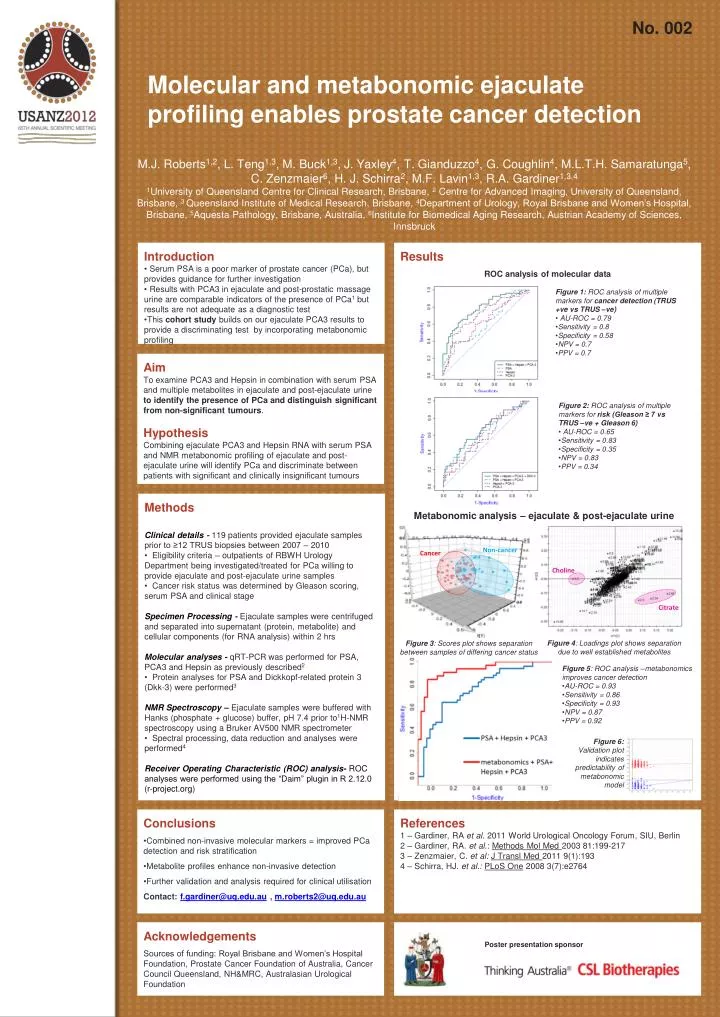
No. 002. Molecular and metabonomic ejaculate profiling enables prostate cancer detection. M.J. Roberts 1,2 , L. Teng 1,3 , M. Buck 1,3 , J. Yaxley 4 , T. Gianduzzo 4 , G. Coughlin 4 , M.L.T.H. Samaratunga 5 , C. Zenzmaier 6 , H. J. Schirra 2 , M.F. Lavin 1,3 , R.A. Gardiner 1,3,4

E N D
No. 002 Molecular and metabonomic ejaculate profiling enables prostate cancer detection M.J. Roberts1,2, L. Teng1,3, M. Buck1,3, J. Yaxley4, T. Gianduzzo4, G. Coughlin4, M.L.T.H. Samaratunga5, C. Zenzmaier6, H. J. Schirra2, M.F. Lavin1,3, R.A. Gardiner1,3,4 1University of Queensland Centre for Clinical Research, Brisbane, 2 Centre for Advanced Imaging, University of Queensland, Brisbane, 3 Queensland Institute of Medical Research, Brisbane, 4Department of Urology, Royal Brisbane and Women’s Hospital, Brisbane, 5Aquesta Pathology, Brisbane, Australia, 6Institute for Biomedical Aging Research, Austrian Academy of Sciences, Innsbruck • Introduction • Serum PSA is a poor marker of prostate cancer (PCa), but provides guidance for further investigation • Results with PCA3 in ejaculate and post-prostatic massage urine are comparable indicators of the presence of PCa1 but results are not adequate as a diagnostic test • This cohort study builds on our ejaculate PCA3 results to provide a discriminating test by incorporating metabonomic profiling Results ROC analysis of molecular data • Figure 1: ROC analysis of multiple markers for cancer detection (TRUS +vevs TRUS –ve) • AU-ROC = 0.79 • Sensitivity = 0.8 • Specificity = 0.58 • NPV = 0.7 • PPV = 0.7 • Aim • To examine PCA3 and Hepsin in combination with serum PSA and multiple metabolites in ejaculate and post-ejaculate urine to identify the presence of PCa and distinguish significant from non-significant tumours. • Hypothesis • Combining ejaculate PCA3 and Hepsin RNA with serum PSA and NMR metabonomic profiling of ejaculate and post-ejaculate urine will identify PCa and discriminate between patients with significant and clinically insignificant tumours • Figure 2: ROC analysis of multiple markers for risk (Gleason ≥ 7 vs TRUS –ve + Gleason 6) • AU-ROC = 0.65 • Sensitivity = 0.83 • Specificity = 0.35 • NPV = 0.83 • PPV = 0.34 • Methods • Clinical details - 119 patients provided ejaculate samples prior to ≥12 TRUS biopsies between 2007 – 2010 • Eligibility criteria – outpatients of RBWH Urology Department being investigated/treated for PCa willing to provide ejaculate and post-ejaculate urine samples • Cancer risk status was determined by Gleason scoring, serum PSA and clinical stage • Specimen Processing - Ejaculate samples were centrifuged and separated into supernatant (protein, metabolite) and cellular components (for RNA analysis) within 2 hrs • Molecular analyses -qRT-PCR was performed for PSA, PCA3 and Hepsin as previously described2 • Protein analyses for PSA and Dickkopf-related protein 3 (Dkk-3) were performed3 • NMR Spectroscopy – Ejaculate samples were buffered with Hanks (phosphate + glucose) buffer, pH 7.4 prior to1H-NMR spectroscopy using a Bruker AV500 NMR spectrometer • Spectral processing, data reduction and analyses were performed4 • Receiver Operating Characteristic (ROC) analysis- ROC analyses were performed using the “Daim” plugin in R 2.12.0 (r-project.org) Metabonomic analysis – ejaculate & post-ejaculate urine Non-cancer Cancer Choline Citrate Figure 4: Loadings plot shows separation due to well established metabolites Figure 3: Scores plot shows separation between samples of differing cancer status • Figure 5: ROC analysis –metabonomics improves cancer detection • AU-ROC = 0.93 • Sensitivity = 0.86 • Specificity = 0.93 • NPV = 0.87 • PPV = 0.92 Figure 6: Validation plot indicates predictability of metabonomic model • Conclusions • Combined non-invasive molecular markers = improved PCa detection and risk stratification • Metabolite profiles enhance non-invasive detection • Further validation and analysis required for clinical utilisation • Contact: f.gardiner@uq.edu.au , m.roberts2@uq.edu.au References 1 – Gardiner, RA et al. 2011 World Urological Oncology Forum, SIU, Berlin 2 – Gardiner, RA. et al.: Methods Mol Med 2003 81:199-217 3 – Zenzmaier, C. et al: J Transl Med 2011 9(1):193 4 – Schirra, HJ. et al.:PLoS One 2008 3(7):e2764 Acknowledgements Sources of funding: Royal Brisbane and Women’s Hospital Foundation, Prostate Cancer Foundation of Australia, Cancer Council Queensland, NH&MRC, Australasian Urological Foundation Poster presentation sponsor