Download
1 / 108
1.16k likes | 1.94k Views
UPDATE ON DIABETES MANAGEMENT. Naushira Pandya M.D., CMD Associate Professor and Chair Nova Southeastern University College of Osteopathic Medicine Ft. Lauderdale, Florida. Objectives. Address the epidemiology and disease burden of diabetes in long-term care

E N D
UPDATE ON DIABETES MANAGEMENT Naushira Pandya M.D., CMD Associate Professor and Chair Nova Southeastern University College of Osteopathic Medicine Ft. Lauderdale, Florida
Objectives • Address the epidemiology and disease burden of diabetes in long-term care • Review existing geriatric guidelines on the care of elders with diabetes • Explore existing practices by long-term care providers • Evaluate the management and risks of hypoglycemia • Facility management of diabetes and the role of the Medical Director
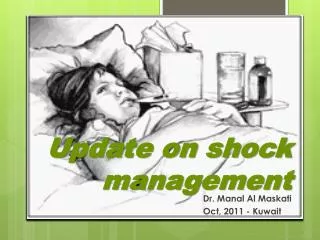
Duration of Diabetes, Life-Years Lost, and Quality-Adjusted Life-Years Lost Among Females Narayan K. et al., JAMA 2003; 290:1884-1890.
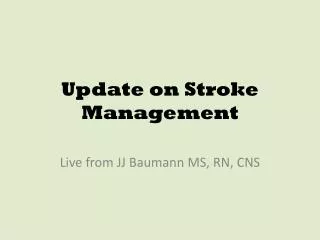
INCREASED MORTALITY IN ELDERS WITH DIABETES Standardized mortality ratio in 131,535 US elders with diabetes Versus general US population aged >65y Bertoni, Krop at al. Diabetes Care;25(3):2002
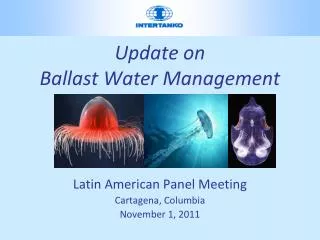
Prevalence of Diabetes in Nursing Homes 40 30 20 10 0 32 30.6 % 14 13.4 9.9 7.2 Mooradian 1988 Grobin 1989 Funnell 1995 Benbow 1997 Sinclair 1997 SLU 2000
The Scope of the Problem in LTC • Diabetes is associated with increased fall prevalence in LTC Maurer MS et al. J Gerontol 60(9);2005 • Diabetes associated with higher mortality in women (RR 2.42) Keily DK. JAMDA 1(1); 2000 • Blacks and Hispanics have lower rates of antidiabetic medication use Ethnicity and Disease 15(2);2005 • Higher rates of cardiovascular disease and depression • Greater degree of functional impairment and dependancy
Burden of Diabetes in LTC • Analyses of nursing home residents with diabetes at admission. Travis, Shirley S. Buchanan, Robert J. Wang, Suojin. Kim, MyungSuk.Journal of the American Medical Directors Association. 5(5):320-7, 2004 Sep-Oct. • All admission assessments in the MDS recorded throughout the United States during 2002 to identify 144,969 residents with diabetes, or 26.4% of all admissions. • Only approximately one fourth of residents with diabetes were projected to have stays in the facility of 90 days or less when admitted. • Heart and circulatory comorbidities were common among residents with diabetes at admission, as was depression. • More than half of residents with diabetes were in pain at admission. .
Burden of Diabetes in LTC…. • A majority of residents with diabetes were either totally dependent or required extensive assistance in the self-performance of many ADLs • More than one third were at least moderately impaired in cognitive performance. • CONCLUSIONS: Residents with diabetes could be one of the most "heavy care" groups in nursing facilities, as demonstrated by their levels of functional disability and prevalence of serious comorbid conditions. • The care provided to residents with diabetes should address depression, pain, and low rates of advance care planning.
Geriatric syndromes more prevalent in persons with diabetes • Polypharmacy • Depression • Cognitive impairment • Urinary incontinence • Injurious falls • Pain
ADDITIONAL COMPLICATIONS OF DIABETES IN FRAIL ELDERLY • Increased susceptibility to infections • Delayed wound healing • Worsening cardiac ischemia/ silent ischemia • Recurrent CHF • Oral dryness, infections, burning, caries, periodontal disease • Urinary retention, UTI’s • Weight loss
Diabetes and cognitive decline? • Several case controlled and population-based studies have shown a clear relationship between diabetes, cognitive decline, and dementia (Framingham, AWARE,Rotterdam, Honolulu Heart Study, CV Health study) • Diabetes and HTN positively associated with cognitive decline over 6 yr in 47-70 yr olds independent of smoking, carotid intimal wall thickness, lipid levels • Interventions aimed at diabetes and HTN below age 60 may lessen the burden of cognitive impairment in later life • Mechanism (other than overt CVA) is probably demyelination, microinfarction in the white matter, and cortical atrophy • LTC study (Tariot JAGS Apr 1999); diabetics more likely to have a diagnosis of vascular dementia than non-diabetics
Depression and Diabetes Geriatric Depression Score Diabetes and Outcomes Rosenthal & Morley, Diabetes Care, 1998. No Yes P Mortality 7.4 15.8 <0.001 Hospitalization 6.7 9.2 <0.001
Diabetes Mellitus is Associated with Increased Likelihood of Developing Pressure Ulcers Brandeis et al. Adv in Wound Care 8:18-25, 1995. Spector. J Invest Dermat 102:425-55, 1994. Brandeis et al. J Am Geriatr Soc 42:388=93, 1994. Early decrease in skin blood flow in response to locally applied pressure in diabetic subjects. Diabetes 51(4). April 2002
REASONS FOR MAINTENANCE OF EUGLYCEMIA IN DIABETICS • Prevention of hyperglycemic comas • Prevention of long term complications • Prevention of fluid and electrolyte imbalance • Prevention of glucose toxicity 1.Accelerated aging 2.Trace mineral deficiency 3.Infection 4.Dehydration 5.Incontinence/nocturia 6.Pain
Summary of Revisions to Standards of Medical Care for Diabetes (ADA)Diabetes Care 29:S3 2006 • Assessment of glycemic control • Use of point-of-care testing for HbA1c (A1C) allows for timely decisions on therapy changes, when needed (E) • Glycemic goals • The A1C goal for patients in general is <7% (B) • The A1C goal for the individual patient is an A1C as close to normal (<6%) as possible without significant hypoglycemia (E) • Nephropathy • To reduce the risk of nephropathy, protein intake should be limited to the Recommended Dietary Allowance (RDA) (0.8 g/kg) in those with any degree of chronic kidney disease (CKD) (B) • Serum creatinine should be measured at least annually for the estimation of glomerular filtration rate (GFR) in all adults with diabetes regardless of the degree of urine albumin excretion. The serum creatinine alone should not be used as a measure of kidney function but rather used to estimate GFR and stage the level of CKD (E)
Guidelines for Improving the Care of theOlder Person with Diabetes MellitusCalifornia Healthcare Foundation/American Geriatrics Society Panel on ImprovingCare for Elders with Diabetes • For older persons, target HB A1C(A1C) should be individualized. • A reasonable goal for A1C in relatively healthy adults with good functional status is 7% or lower. • For frail older adults, persons with life expectancy of less than 5 years, and others in whom the risks of intensive glycemic control appear to outweigh the benefits, a less stringent target such as 8% is appropriate. (IIIB)
Wisconsin Essential Diabetes MellitusCare GuidelinesRevised 2004
Glucose Tolerance Categories FPG 2-h PPG (OGTT) Plasma glucose (mg/dL) 240 Diabetes Mellitus 220 200 Diabetes Mellitus 180 IGT 160 140 126 120 IFG Normal 100 Normal 80 60 American Diabetes Association. Diabetes Care. 2004;27(suppl 1):S5-S10 8
Impaired Glucose Tolerance (IGT) 2-h PG on OGTT 140 but 200 mg/dL Predicts increased risk of diabetes and cardiovascular disease Impaired Fasting Glucose (IFG) FPG 100 but 126 mg/dL Predicts increased risk of diabetes and micro- and macrovascular complications IFG and IGTIntermediate Between Normal and Diabetes 9
DIABETES AND DIET • There is no longer a “diabetic diet” • Consistent carbohydrate content, portion size, increased fiber, and nutritional adequacy are important • Avoid dietary restrictions (especially fat)- reduces quality of life - may lead to undernutrition in patients with depression, dependancy, chewing difficulty, and functional disability • “No concentrated sweets” diet is inappropriate - does not significantly improve glycemic control. Tariq, J Am Diet Assoc 2001, 101(12) • Adjust oral agents and/ or insulin to balance food consumption
The Role of Special Supplements- GLUCERNA Glucose concentration at 120 min after interventions. N=14 (single blind cross over trial of Ensure High Calcium and Glucerna in young adults) Diab Obes Metab;May 2006 Insulin sensitivity after interventions. Older adults preferred the flavor of Glucerna SR vs. Resource Support in another study. N=456 Nutricion Hospitalaria; Sept 2004 Neutral on glucose and triglyceries in 63 tube-fed hospitalized pts J Parent Gut Nutrition;Jan-Feb 2005
Class Agents Secretagogue Sulfonylureas Repaglinide, nateglinide Biguanide Metformin α-Glucosidase inhibitor Acarbose, miglitol Glitazone (TZD) Pioglitazone, rosiglitazone DPPIV inhibitors Sitagliptan Oral Antihyperglycemic Agentsfor Type 2 Diabetes
Antihyperglycemic AgentsMajor Sites of Action Glitazones -Glucosidase inhibitors – Plasma glucose + Carbohydrate absorption Glucose uptake GI tract Muscle/Fat + Glucose production – – Injected Metformin + Liver insulin – Insulin secretion + Secretagogues Pancreas
Oral Antihyperglycemic MonotherapyMaximum Therapeutic Effect on A1C Nateglinide Acarbose Repaglinide Rosiglitazone Pioglitazone Glimepiride Glipizide GITS Metformin -1.0 -1.5 -2.0 0 -0.5 Reduction in A1C (%) Diabetes Care. 2000;23:202-207; Precose (acarbose) package insert; Drugs. 1995;50:263-288; J Clin Endocrinol Metab. 2001;86:280-288; Diabetes Care. 2000;23:1605-1611; Diabetes Care. 1996;19:849-856; Diabetes Care. 1997;20:597-606; Am J Med. 1997;102:491-497
Mechanism of Action of Sitagliptin Glucose dependent Insulin (GLP-1andGIP) Glucose uptake by peripheral tissue Ingestion of food Pancreas Release of active incretins GLP-1 and GIP Beta cells Alpha cells GI tract Blood glucose in fasting and postprandial states Glucose- dependent X JANUVIA (DPP-4 inhibitor) DPP-4 enzyme Hepatic glucose production Glucagon (GLP-1) Inactive GLP-1 Inactive GIP • Incretin hormones GLP-1 and GIP are released by the intestine throughout the day, and their levels in response to a meal. Concentrations of the active intact hormones are increased by JANUVIA™ (sitagliptin phosphate), thereby increasing and prolonging the actions of these hormones.
Clinical Pharmacology of Sitagliptan(JANUVIA™) • Pharmacodynamics • Leads to inhibition of DPP-4 activity for a 24-hour period in patients with type 2 diabetes, resulting in: • 2- to 3-fold in circulating levels of active GLP-1 and GIP • glucagon concentrations • responsiveness of insulin release to glucose • plasma levels of insulin and C-peptide • fasting glucose and glucose excursion after an oral glucose load or a meal • In healthy subjects, sitagliptan did not lower blood glucose or cause hypoglycemia
Indications and Usage of Sitagliptan • Monotherapy • Adjunct to diet and exercise to improve glycemic control in patients with type 2 diabetes mellitus • Combination therapy • To improve glycemic control in combination with metformin or a PPAR agonist (e.g., thiazolidinediones) when the single agent alone with diet and exercise does not provide adequate glycemic control • Important limitations of use • Sitalgliptan should not be used in patients with type 1 diabetes or for the treatment of diabetic ketoacidosis PPAR=peroxisome proliferator-activated receptor gamma.
S e c t i o n 2 Dosage and Administration Patients With Renal Insufficiency*,† Assessment of renal function is recommended prior to initiationof JANUVIA and periodically thereafter. *JANUVIA can be taken with or without food. †Patients with mild renal insufficiency—100 mg once daily. ‡ESRD = end-stage renal disease requiring hemodialysis or peritoneal dialysis.
Summary ofOral Antihyperglycemic Agents • Five major classes of oral agents acting at different sites are available • Fasting and preprandial glucose are reduced by sulfonylureas, repaglinide, metformin, and glitazones (TZDs), with lesser effects on postprandial increments • Postprandial glucose increments are reduced best by -glucosidase inhibitors and nateglinide • A1C reductions are similar using sulfonylureas, metformin, and glitazones • Secondary failure to monotherapy routinely occurs
Algorithm on treatment of T2DM based on degree of hyperglycemia
Algorithm based on pathology for T2DM patients with mild or moderate hyperglycemia after diet and exercise
Pathophysilogi- cally based treatment algorithm for T2DM patients with severe hyperglycemia
American Heart Association and American Diabetes Assoc algorithm for TZD use and Heart failure
Efficacy of Oral AntihyperglycemicsDeclines With Time • A1C rises at ~0.2% to 0.3% yearly on stable therapy • This rate is the same as for diet alone, sulfonylureas, and metformin • -Cell function declines at the same rate with all these treatments • Combination treatments are routinely needed UKPDS Group. Diabetes. 1995;44:1249-1258; Turner RC et al. JAMA. 1999;281:2005-2012
Improved glycemic control over conventional therapy was attained with either insulin initiation or early addition of insulin to sulfonylureas if glycemic targets were not met
WHEN TO USE INSULIN IMMEDIATELY • Marked hyperglycemia OR • Significant weight loss OR • Severe symptoms OR • > 2+ ketonuria • Diabetic ketoacidosis, hyperosmolar state OR • Severe intercurrent illness, surgery (CABG)
Insulin Preparations Class Agents Human insulins Regular, NPH Insulin analogues Aspart, glulisine, lispro, glargine Premixed insulins Human 70/30, 50/50 Humalog mix 75/25 Novolog mix 70/30
2 3 4 5 6 7 8 9 12 13 14 15 16 17 18 19 20 21 22 23 24 0 1 10 11 Action Profiles of Insulin Analogues Aspart, glulisine, lispro 4–6 hours Regular 6–8 hours Plasma insulin levels NPH 12–20 hours Ultralente 18–24 hours Glargine 24 hours Hours
Which basal insulin? Once daily bedtime NPH or glargine systematically titrated to give fasting glucose <100mg/dl achieves similar glycemic control
Significant reductions in nocturnal hypoglycemia in patients treated with insulin glargine compared to NPH insulin
Efficacy and Safety of Insulin Glargine in Elderly Patients: A1C Levels at Week 24 T2DM -1.54 -1.13 -1.01 A1C (%) ≥ Age (y) No statistically significant differences was found between groups at baseline. P<0.01, <65 vs 65-74 years and <65 adjusted for study arms, body mass index, baseline glycosylated hemoglobin (A1C), use of sulfonylurea and metformin, and thiazolidinedione discontinuation at week 24. Abstracts of the 66th Scientific Sessions of the ADA. Diabetes. 2006; 55(suppl 1): A114 Abstract 480-P. Study: GOAL A1C
Insulin Glargine Versus Premixed Insulin in Elderly Patients: A1C Reduction T2DM Insulin Glargine + OADs Premixed Insulin P=0.003 Janka H, Plewe G, and Busch K. J Am Geriatr Soc.2007;55:182-188.
Insulin Glargine Versus Premixed Insulin in Elderly Patients: Patients Achieving Glycemic Control T2DM P=0.0057 Janka H, Plewe G, and Busch K. J Am Geriatr Soc.2007;55:182-188.
Insulin Glargine Versus Premixed Insulin in Elderly Patients: Hypoglycemic Episodes T2DM P=0.01 P=0.26 Janka H, Plewe G, and Busch K. J Am Geriatr Soc.2007;55:182-188
Initiation of basal insulin • Continue oral agent if tolerated and no specific contraindications • Keep metformin dose up to 2000mg/d • Reduce pioglitazone to 15-30mg/g and roziglitazone to 2-4mg/d • Reduce sulfonylurea to 50% of dose (if glyburide, substitute to different sulfonylurea or meglitinide) • Start insulin 10 units • Glargine at bedtime or same time • NPH at bedtime or twice daily • Detemir at bedtime or twice daily
What dose of insulin? • Basal insulin: start 10 U/d bedtime NPH or Glargine (whatever time preferred) • Titration: e.g., in Treat-to-Target trial FPG goal was <100 m/dl and doses titrated weekly • Bolus (prandial) insulin: start rapid acting analog 0.1 U/kg
Advance Basal Insulin plus Prandial Insulin at Main Meal • Continue basal insulin weekly self-titration • Consider adding prandial insulin at main meal • if FPG consistently lower than 100mg/dl and HbA1c remains higher than 7% • Cannot increase further basal insulin without hypoglycemia • Basal insulin dose is more than 100 units
Riddle MC. Endocrinol Metab Clin North Am. 1997;26:659-677 Management of HyperglycemiaAdvancing to Two Injections Consider when FPG acceptable but A1C >7% on one injection • Insulin options • To bedtime NPH, add morning NPH • To suppertime premix, add morning premix • To glargine, add regular, aspart, or lispro to mainmeal • Oral agent options • Usually stop sulfonylureas • Continue metformin for weight control? • Continue glitazones for glycemic stability?
1200 2400 1800 0800 0600 0600 Split-Mixed RegimenHuman Insulins NPH Regular NPH Regular U/mL 100 B L D 80 Normal pattern 60 40 20 Time of day B=breakfast; L=lunch; D=dinner