Download
1 / 28
280 likes | 639 Views
To Admit or Not to Admit. Patient. Presents. The Decision Seems Easy…. Admit as Inpatient. Treat as Outpatient. Admit as Inpatient. But It’s Much More Complicated. Office Follow-up. Specialty Clinic Follow-up. Treat as Outpatient. Outpatient Procedure. SNF Follow-up.

E N D
Patient Presents The Decision Seems Easy… Admit as Inpatient Treat as Outpatient
Admit as Inpatient But It’s Much More Complicated Office Follow-up Specialty Clinic Follow-up Treat as Outpatient Outpatient Procedure SNF Follow-up Diagnostic Testing Observation
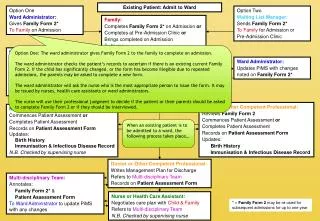
Patient Presents Patient Status Options Admit as Inpatient Outpatient Observation Outpatient Procedure and/or Followup
Effects of Unnecessary Admissions • Costs Medicare the largest proportion of erroneous payments • One-day stay admissions are target area for potential payment errors in MO • OIG has taken notice
Why It Matters • Majority of error payment amount (~$1.6B) may be attributed to lack of medical necessity • Nearly 80% of all admission denials were short stays (1-3 days) • MO’s net error payment FY2005 estimated at $47M; majority of which may be attributable to unnecessary IP admissions
Why It Matters • Why does it matter to the patient? • Why does it matter to the hospital? • Why does it matter to the physician?
Admit as Inpatient • Treatment longer than 24 hours expected • Outpatient treatment has not been effective • Inpatient-only procedure necessary • Continuous monitoring necessary
Inpatient Admission Considerations • Severity of presenting signs and symptoms • Predictability of the clinical course • Existence of comorbid conditions which may negatively impact course • Potential for complications • Services required upon presentation • Diagnostic procedures available
Inpatient Admission Documentation • Inpatient admission order with date and time • Clinical documentation supporting medical necessity • No “back-dating” is allowed
What are Observation Services? • Services furnished by a hospital including: • use of bed • periodic monitoring by staff • requires physician order • Reasonable and necessary • evaluate outpatient condition • determine inpatient admission need
Why Observation Services? • Determines need for inpatient admission • Rapid response to treatment is expected • Patient has unusually prolonged recovery period following an OP procedure
Points of Entry for Outpatient Observation • Admission from emergency department • Direct admission • Outpatient department(s)
ObservationDocumentation • Observation admission order with date and time • Assessment of patient risk to determine benefit from observation care • Timed and signed admission notes, progress notes and discharge notes
Observation Services Not Covered • Services not reasonable or necessary for diagnosis or treatment of patient • Services provided for convenience of patient, family or physician • Services covered under Part A • Services that are part of another Part B service • Standing orders for observation after OP surgery • Custodial care
Condition Code 44 Policy • Medicare payment policy that allows inpatient admission change to outpatient when: • Change in status made prior to discharge • The hospital has not submitted Medicare claim for inpatient admission • Physician concurs with decision to change status • Physician’s concurrence is documented in medical record
Chest Pain • Process of elimination to determine chest pain is not cardiac in origin based on: • Symptoms • ECG • Enzymes • Possible early stress testing
Chest Pain Evaluation • New onset symptoms may be consistent with ischemic heart disease butnot associated with ECG changes or convincing evidence of unstable ischemic heart disease at rest or with minimal exertion • Known CAD but symptoms do not suggest true worsening • Observation beneficial because etiology of symptoms is unclear
Chest Pain Case Study #1 • 84-year-old female, PMH=CABG, presented to ED with intermittent chest pain x1 wk which increases on deep inspiration; Initial enzymes & ECG unremarkable; pain resolved prior to admission • Patient admitted with atypical pain in setting of prior CABG; Plan=serial ECGs & enzymes • Admission to observation status appropriate
Chest Pain Case Study #2 • 63-year-old female, PMH=CAD with prior MI 1990s, HTN, CVA; presented to ED with chest pain, sharp, retrosternal, dyspnea & diaphoresis; pain increases with minimal exertion; pain relieved w/rest & NTG; pain recurred several times in ED; SBP >100; • Initial impression=unstable angina, r/o MI
Chest Pain Case Study #2 (cont’d) • Initial enzymes WNL, ECG=non-specific ST- T changes; admitted to telemetry unit for r/o MI protocol & stress perfusion w/dipyridamole, which showed anterior wall ischemia; • New onset angina in setting of prior MI; IP admission appropriate
Syncope & Collapse Case Study #3 • 70-year-old female presented to the ED “knees gave out & I fell to floor…hit back of head”; denies LOC, dizziness, lightheadedness, chest pain, & N/V; PMH=DM; vital signs WNL w/no findings on exam; BS=189; Enzymes nl; ECG WNL; head CT negative
Syncope & Collapse Case Study #3 (cont’d) • Questionable pre-syncope of unknown etiology; admit to monitor for arrhythmias or other neuro signs • Admission to observation status appropriate
Syncope & Collapse Case Study #4 • 65-year-old male came to ED with 3 syncopal episodes each lasting several seconds, occurring over 18-hr period; H&P unremarkable; ECG=bradycardia of 54bpm & 18 sec pause; ECHO=WNL; • Appropriate IP admission for pacemaker insertion and postprocedure monitoring
Dehydration Case Study #5 • 92-year-old female presented to the ED with weakness x2 days & difficulty getting in & out of bed; no fever, dizziness, nausea, vomiting, diarrhea; PMH=HTN, dementia, recent tx for UTI; Sodium=132; decreased oral intake; HR >100; postural SBP drop >30 • Tx plan=BP meds held; IVFs 100/hr; po antibiotics
Dehydration Case Study #5 (cont’d) • Meets severity of illness (InterQual endocrine/metabolic) but doesn’t meet intensity of service • Per PR review---documentation indicates status of dehydration could reasonably be expected to improve within 24-hour period; overnight monitoring in observation status appropriate.
Observation or Inpatient? Hospitalization required? Yes 24 hours adequate to evaluate, treat or respond? No No Inpatient Yes No acute hospital care Observation
References • Federal Register, Nov. 10, 2005 • Medicare Claims Processing Manual • Medicare Benefit Policy Manual • Mutual of Omaha • InterQual® admission screening criteria • HPMP Compliance Workbook