Download
1 / 22
220 likes | 374 Views
First in Human Trial of a Poly(ADP- ribose) Polymerase (PARP) Inhibitor MK-4827 in Advanced Cancer Patients with Anti-tumor Activity in BRCA -Deficient and Sporadic Ovarian Cancers. SK Sandhu 1,2 , R Wenham 3 , G Wilding 4 , M McFadden 5 , L Sun 5 ,

E N D
First in Human Trial of a Poly(ADP-ribose) Polymerase (PARP) Inhibitor MK-4827 in Advanced Cancer Patients with Anti-tumor Activity in BRCA-Deficient and Sporadic Ovarian Cancers SK Sandhu1,2, R Wenham3, G Wilding4, M McFadden5, L Sun5, C Toniatti5, M Stroh5, C Carpenter5, J de-Bono1,2, WR Schelman4 1.Drug Development Unit, Royal Marsden NHS Foundation Trust, Sutton, UK 2.The Institute of Cancer Research, Sutton & London, UK 3.H. Lee Moffitt Cancer Center & Research Institute, Tampa, FL, US 4.University of Wisconsin Carbone Cancer Center, Madison, WI, US 5..Merck & Co., Inc., Whitehouse Station, New Jersey, USA
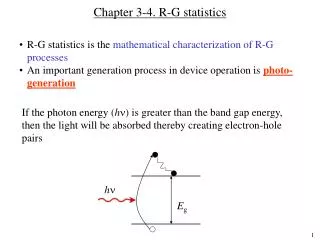
PARP Inhibition and Tumor-Selective Synthetic Lethality Normal S Phase DNA replication SSB BER PARP DNA replication fork arrest and collapse PARP Unrepaired SSB Normal BRCA1& BRCA2 function BRCA1 or BRCA2 deficiency HR-based repair HR-based repair Reliance on error prone DNA repair Genomic stability Cell viability DNA damage Cell death Farmer H et al, Nature, 2005;434:917-921 Bryant HE et al, Nature, 2005,434:913-917
Tumor-Selective Synthetic Lethality DNA damage } Germline mutation Somatic mutation Epigenetic silencing BER PARPi BRCA1 Ovarian Breast Germline mutation Somatic mutation Epigenetic silencing Stalled replication forks DNA DSB BRCA2 ATM Normal cell or heterozygote for HR HR deficient tumor FANCD2 FA complex HR repair No HR repair RAD51 Endometrial Breast Prostate Glioblastoma PTEN loss } Cell viability Cell death Turner N, et al. Nat Rev Cancer.2004;4:814-9 Mendes-Pereira AM, et al. EMBO Mol Med. 2009;1:315-22 B. Hennessy, et al. J CO 27:15s, 2009 (suppl; abstr 5528) Esteller M, et al.J Natl Cancer Inst.2000;92:564-569 Farmer H, et al. Nature, 2005;434:917-921 Bryant HE, et al. Nature, 2005;434:913-917 McCabe N, et al. Cancer Res. 2006;66:8109-15 Press JZ , et al. BMC Cancer 2008;8:1-12
PARP-1 PARP-2 PARP-3 v-PARP TANK-1 3.8 2.1 1300 330 570 IC50 C O N H 2 N H N ( S ) N MK-4827 • Highly selective, PARP-1/2 inhibitor • In vitro monotherapy efficacy: • BRCA-1 or BRCA-2 deficient • CC50 = 10-90 nM {>10-fold selectivity over BRCA-wt cells (CC50 ≥ 1500 nM)} • ATM inactivation • CC50 = 100-300 nM • PTEN deletion • CC50 = 100-800 nM
Study Objectives • Primary objectives • Safety and tolerability, dose limiting toxicities (DLT), maximum tolerated dose (MTD), recommended phase 2 dose (RP2D) • Secondary objectives • Pharmacokinetic (PK) and pharmacodynamic (PD) profile • Preliminary assessment of anti-tumor activity in patients with cancers likely to have a HR DNA repair defects
Methods • First in human, open-label, Phase I study • Royal Marsden NHS Foundation Trust, Moffitt Cancer Center, University of Wisconsin Carbone Cancer Center • Oral once daily dosing; two part study • Dose escalation: Enrichment for BRCA1 and BRCA2 mutation carriers • Dose expansion: Sporadic platinum resistant high grade serous ovarian cancer & castration resistant prostate cancer (CRPC)
Inclusion and Exclusion criteria • Inclusion criteria • Over the age of 18 • Advanced malignancy • Confirmed histological diagnosis • Informed consent • Adequate organ function • ECOG PS of ≤ 2 • Exclusion criteria • Receiving another investigational agent • Hypersensitivity to study drug or analogues • Prior treatment with a PARP inhibitor • Uncontrolled medical condition
Part A: Dose escalation & MTD confirmation 59 patients enrolled Enriched for BRCA1/2 mutation carriers Safety PK-PD relationship Part B: Dose expansion Safety PK-PD relationship Anti-tumor activity in sporadic tumors MK4827 Phase I Study: Results 400 mg n=6 300 mg n=9 MTD cohort 290 mg n=5 Sporadic platinum resistant high grade serous ovarian cancer* n=30 210 mg n=6 150 mg n=6 110 mg n=5 Sporadic castration resistant prostate cancer* n=20 80 mg n=6 60 mg n=7 40 mg n=3 30 mg n=6 * High likelihood of having HR DNA repair defect
Dose Limiting Toxicities (DLT) • Thrombocytopenia was dose limiting • MTD = 300mg QD
Preliminary Pharmacokinetic (PK) Profile • Dose proportional pharmacokinetics • Three-fold accumulation in AUC0-24, Cmax and C24 over the 1st cycle • Steady state achieved following one 21-day cycle • Terminal half-life is 37-42 hours
Pharmacodynamic (PD) Profile 140 120 100 80 %PARP activity (relative to baseline) 60 50 40 20 60mg 40 mg 80 mg 30 mg 150 mg 210 mg 290 mg 400 mg 110 mg N=18 patients Dose • Functional PARP activity in PBMCs: trough levels on C1D21 or C2D1 • Percent inhibition calculated using the mean of 2 baseline samples
Nuclear staining γH2AX foci Gamma H2AX Foci Induction in Tumor Biopsy Cycle 1 day 22 MK4827 300mg Cycle 1 day1, predose MK4827 300mg • Paired fresh frozen tumor biopsy in a BRCA2 mutation carrier with breast cancer • Stained for gamma H2AX foci pre and post treatment
+ 400mg + Increasing dose 300mg + 290 mg + 210mg + 150mg 110mg + 110mg + 80mg + 60mg 110mg + Increasing dose 60mg 60mg 40mg Stable disease for ≥ 120 days Partial response by RECIST criteria GCIG CA125 partial response + Ongoing treatment ■ BRCA1 or BRCA2 mutation carrier MK-4827 Anti-Tumor Efficacy Patients on 400mg were dose reduced to 300mg in C2
Hereditary Ovarian and Breast Cancer: Preliminary Response Data
Day61 Baseline 14mm 24.5mm Hereditary Breast and Ovarian Cancer Baseline BRCA1 mutation carrier Baseline Day46 Baseline Baseline Day98 71mm 30mm BRCA2 mutation carrier BRCA2 mutation carrier
Hereditary Ovarian Cancer: CA125 Response GCIG CA125 response 95% reduction MK-4827 290mg
Sporadic Ovarian Cancer Patient Baseline Day 101 • FIGO Stage 3B high grade serous ovarian cancer; No family history* • Five prior lines of platinum-based chemotherapy; last platinum free interval of 7 months • 357 days on MK4827, ongoing PR by RECIST & GCIG CA125 criteria * Studies of HR DNA repair proficiency ongoing
Sporadic Ovarian Cancer: Ca125 Response GCIG CA125 response 94% reduction Maintained PR by RECIST criteria MK-4827 60mg MK-4827 increased from 60mg to 210mg
Conclusions • Safety • MK-4827 was well tolerated • Continuous oral administration at 300mg is the MTD • PK • Dose proportional pharmacokinetic profile • PD • Proof of mechanism has confirmed PARP inhibition from doses of ≥ 80mg • Compelling anti-tumor activity observed • Heavily pre-treated BRCA1 and BRCA2 mutation carriers • Preliminary anti-tumor activity seen in sporadic cancers
Patients and their families DDU, Royal Marsden Hospital Stan Kaye Richard Baird Martin Forster Elizabeth Sheridan Jen Lewis Alima Rahman The Institute of Cancer Research Alan Ashworth Chris Lord H. Lee Moffitt Cancer Center & Research Institute Irene Williams-Elson University of Wisconsin Carbone Cancer Center Jennifer Heideman Merck & Co. Inc Judith Allen ASCO Cancer Foundation Acknowledgements



![[4] [5] [3] [2] [4]](https://cdn1.slideserve.com/2491770/slide1-dt.jpg)