Download
1 / 20
250 likes | 332 Views
Pathogenesis of Hypertension: Genetic and Environmental Factors. Mohammad Saifur Rohman, MD. PhD. FIHA. Dept. Cardiology and Vascular Medicine Brawijaya University/ dr. Saiful Anwar Hospital, Malang. Clinical Principles

E N D
Pathogenesis of Hypertension: Genetic and Environmental Factors Mohammad Saifur Rohman, MD. PhD. FIHA. Dept. Cardiology and Vascular Medicine Brawijaya University/ dr. Saiful Anwar Hospital, Malang
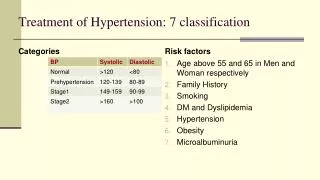
Clinical Principles • A clearer understanding of the pathogenesis of hypertension will probably lead to more highly targeted therapies and to greater reduction in hypertension-related cardiovascular disease morbidity than can be achieved with current empirical treatment.
Physiologic Principles • More than 90% of cases of hypertension do not have a clear cause. • Hypertension clusters in families and results from a complex interaction of genetic and environmental factors. • The hypertension-related genes identified to date regulate renal salt and water handling.
Major pathophysiologic mechanisms of hypertension include activation of the sympathetic nervous system and renin–angiotensin–aldosterone system. • Endothelial dysfunction, increased vascular reactivity, and vascular remodeling may be causes, rather than consequences, of blood pressure elevation; increased vascular stiffness contributes to isolated systolic hypertension in the elderly.
Essential hypertension • Collision of an modern lifestyle with Paleolithic genes • Lifestyle : Intake vs. output • High salt intake, calorie excess, social stress • Less activity, low potasium diet • Genes: • Poligenic • No straightforward phenotypic effect
Environment / Individual shared: Diet: Na, K, Ca, calories, Alcohol, Caffeine, Fat, etc. Oral contraceptives Stress Physical activity Lower Education Glucocorticoidremidiablealdosteronism Na-K con trasporter Angiotensin Kalirein
Genotype environment Observed expression Ion transport genes Na, K, Ca, Cl, Mg intake Catecholamine genes Stress, inactivity Brown adipose tissue gene Fat and calorie intake Impaired membrane transport Altered catecholamine receptors and enzymes Coupled protein conductance in brown adipose tissues
Phenotype Clinical feature Disturbed ion-fluid balance Altered sympathetic balance Decreased postprandial thermogenesis Altered hemodynamic regulation Altered cardiac output and/or vascular resistance High percentage of extra calories converted to fat
Fluid Volume Pathogenesis of Hypertension Excess sodium intake Reduced Nephron number Stress Genetic Alteration Endothelium derived factors Obesity Blood Pressure = Cardiac Output (CO) X Peripheral Resistance (PR) Hypertension Increased CO and/or Increased PR Sympathetic nervous overactivity Renal Sodium retension Decreased Filtration surface Renin Angiotensin Excess Hyperinsulinemia Cell membrane alteration Venous Constriction Preload Contractility Functional Constriction Structural Hypertrophy Autoregulation Kaplan NM, Clinical Hypertension 7th ed. 2002; 63
Consequences Structural Changes in Hypertension Loss of buffering Function Transmits Systolic pressure Wave to small arteries Increased blood pressure Structural changes in compliance arteries Compliance Load on heart Shear stress on Artery wall Endothelial dysfunction Perpetuation of Hypertension Left Ventricular Hypertrophy Predisposes of Atherosclerosis Dzau VJ. Hypertension. 2001;37:1047-1052
Hypertension Leads to Atherosclerosis Hypertension Further rise in blood pressure and Vascular damage ATHEROSCLEROSIS Local effects (Prostaglandine, free radicals, etc) Endothelial damage Platelet deposition Mitogenic and migration factors Myointimal proliferation Systemic effects (Renin-angiotensin, catecholamine, vasopressin) Pressure natriuresis Hypovolemia Further increase in vasopressors Dzau VJ. Hypertension. 2001;37:1047-1052
Hyperinsulinemia - Hypertension • Insulin Resistance • Hyperinsulinemia • Sodium Retention Increased Na-K ATPase • Increased Intracell. Na • Increased Intracell. Ca • Vasocontric. VSMC • Increased Vasc. Resist. • Hypertension DeFronzo RA, et al. J Clin Invest 1976; 58: 83-90
Contributing Factors to Hypertension in Metabolic Syndromes • Endothelial dysfunction and activation of renin angiotensin aldosteron system • Activation of sympathetic nervous system and increased Cathecolamin • Insulin resistance: Decreased insulin sensitivity 10 uM/m/kg or insulin resistance 30% results in increased 1.7 mmHg systolic pressure and 2.3 mmHg diastolic pressure. Sowers JR. N Eng J Med 2002: 346; 1999-2001. Reaven GM, et al. N Engl J Med 1996: 334; 374-381.