Download
1 / 64
720 likes | 856 Views
Learn about the etiology, clinical features, diagnosis, and diseases presenting as desquamative gingivitis. Explore conditions such as lichen planus, pemphigoid, and more. Understand the systematic approach to diagnosis and available treatments for this oral mucosal manifestation.

E N D
Contents Introduction Etiology Clinical Features Diagnosis Diseases Clinically Presenting As Desquamative Gingivitis Lichen Planus Pemphigoid Mucus Membrane Pemphigoid Pemphigus Chronic Ulcerative Stomatitis Linear IgA Disease Dermatitis Herpetiformis Lupus Erythematosus Erythema Multiforme Drug Eruptions Miscellaneous Conditions Mimicking Desquamative Gingivitis Conclusion
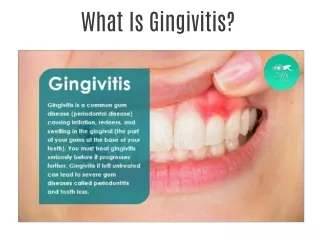
Introduction • Rare nonspecific manifestation of oral mucosa • Prinz (1932)- “chronic diffuse desquamative gingivitis”is a specific disease, characterized by erythema, desquammation and ulceration of the free and attached gingiva • McCarthy and Shklar (1960)-desquamative gingivitis is not a specific disease , but a gingival response associated with a variety of conditions
Etiology • Certain dermatoses • Hormonal influence • Chronic infections • Idiopathic Most important dermatoses • Lichen Planus • Cicatrical Pemphigoid (MMP) • Pemphigus Vulgaris
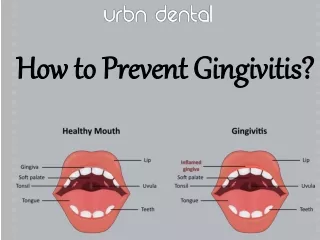
Clinical Features • Gingivae - red, swollen and glossy in appearance • Occasionally multiple vesicles and superficial denuded areas • Nikolsky’s sign • Sensitive gingival tissue – difficulty in eating hot, cold or spicy food
Diagnosis of Desquamative Gingivits Systematic Approach – • Clinical History • Clinical Examination • Biopsy • Microscopic Examination • Immunofluorescence
A Systematic approach is needed to diagnose disease associated with Desquamative gingivitis -
Management 3 factors • Practitioner’s experience • Direct and exclusive responsibility of the treatment e.g., erosive lichen planus which is responsive to topical steroids 2. Systemic impact of the disease • Collaboration with another dectors. e.g., cicatrical pemphigoid where the dentist treats the oral lesions and ophthalmologist deals with ocular lesions
3. Systemic complications of the condition • Only medical practitioner treats the disease e.g., pemphigus vulgaris
1. Lichen Planus • A muco cutaneous condition, an immunological disorder involving T- lymphocytes. • Females affected more than males
Clinical Features • Adults - > 40 years • F:M – 2:1 • Small, angular, flat-topped papules only a few millimeters in diameter • Wickham’s striae – fine, grayish-white lines covering the papules • Commonly involved sites- • Flexor surfaces of wrist • Inner aspect of knees & thighs • Trunk
Types of Lichen Planus - • Chronic Dermatosis- violet papules with pruritis • Oral lesions- Reticular( Wickhamsstriae) Atrophic Bullous & Erosive 3. Gingival lesions- Keratotic Erosive or Ulcerative Vesicular or bullous
Oral Lesions • Reticular type – • Asymptomatic • Bilateral on the posterior region of buccal mucosa • Tongue, gingiva, palate, alveolar mucosa may also be affected • Interlacing white lines
Erosive type – • Usually painful • Atrophic, erythematous and often ulcerated areas • Fine, white radiating striations bordering the atrophic and ulcerated zones • Sensitive to heat, acid and spicy foods
Gingival Lesions Keratotic lesions • Raised white lesions presenting as groups of individual papules, linear or reticular lesions, or plaque like configurations Erosive or Ulcerative lesions • Extensive erythematous areas with a patchy distribution • Exacerbated by slight trauma (e.g., tooth brushing)
Vesicular or Bullous lesion • Raised, fluid-filled lesions which rupture quickly and leave ulceration • Atrophic lesions • Produce epithelial thinning resulting in gingival erythema
Differential Diagnosis • Lichenoid reactions • Leukoplakia • Candidiasis • Pemphigus • Cicatrical pemphigoid • Erythema multiforme • Syphilis • Recurrent aphthae • Lupus erythematosus • Chronic ulcerative stomatitis
Treatment • Keratotic, asymptomatic lesions – no Rx. Regular follow-up • Erosive/bullous/ ulcerative lesions - topical steroids such as 0.05% fluocinonide ointment (Lidex TDS) • In more severe cases, • Intralesional injections of triamcinolone acetonide or • 40 mg of prednisone OD for 5 days, followed by 10-20 mg OD for an additional 2 weeks • Elimination of mechanical trauma or irritants such as sharp filling margins
Alternative to Corticosteroids - • Cyclosporine • Levamisole • Topical human interferon – β • Systemic isotretinoin • Dapsone Non-Drug Therapy • Surgical excision • Cryosurgery • CO2 laser • Ultraviolet radiation • Magnetism
2. Pemphigoid • A number of cutaneous, immune-mediated, subepithelial bullous diseases characterized by a separation of the basement membrane zone (BMZ) • Bullous Pemphigoid (nonscarring & confined to skin) • Mucous Membrane Pemphigoid (scarring & confined to MM) • Pemphigoid Gestationis
Bullo us Pemphigoid (BP) • Chronic, autoimmune, subepidermal, blistering skin disease that rarely involves mucous membranes • Oral involvement occurs in few patients
Clinical Features • > 60 years of age • Generalized, nonspecific rash, commonly on the limbs which may persist for several weeks to several months • Appearance of the vesiculobullous lesions • Vesicles/bullae remain intact for some days or may rupture to leave a raw, eroded area which heals rapidly
Oral Lesions • Vesicles and areas of erosion and ulceration • Gingival tissues - extremely erythematous and may desquamate as a result of even minor frictional trauma
Therapy • Primary Rx - Moderate dose of systemic prednisone • When high doses of steroids are needed or the steroid alone fails to control the disease - Steroid-sparing strategies (prednisone plus other immunomodulator drugs) • For localized lesions of BP - • Topical steroids • Tetracycline with/without nicotinamide
Mucous Membrane Pemphigoid(CicatricalPemphigoid) • Chronic, vesiculobullous autoimmune disorder of unknown origin that predominantly affects the mucous membranes, including the mouth and the oropharynx, the conjunctiva, the nares and the genitalia
Subtypes • Oral pemphigoid • Antiepiligrin pemphigoid • Anti-BP antigen mucosal pemphigoid • Multiple-antigens pemphigoid • Ocular pemphigoid
Clinical Features • Peak age - 40 and 50 years Ocular Lesions • Unilateral conjunctivitis that becomes bilateral within 2 years • Symblepharon - adhesions of eyelid to eyeball • Ankyloblepharon - adhesions at the edges of the eyelids • Narrowing of palpebral fissure
Oral Lesions • Desquamative gingivitis, with areas of erythema, desquamation, ulceration and vesiculation of the attached gingiva • Lesions - vesiculobullous in nature • - persist for 2-3 days • - rupture leaving a raw, eroded bleeding surface • Involvement of the oropharynx - dysphagia
Therapy • Fluocinonide (0.05%) & Clobetasol propionate (0.05%) in an adhesive vehicle TDS for up to 6 months • When confined to gingival tissues - topical corticosteroids • Meticulous oral hygiene • Minimize gingival irritation from any dental prosthesis • If ocular involvement is present - systemic corticosteroids are indicated
3. Pemphigus Vulgaris • Autoimmune bullous disorders that produce cutaneous and mucous membrane blisters • Potentially lethal, chronic condition • 10% mortality rate
Etiology • Diet – controversial • Drugs – Penicillamine Rifampicin Diclofenac • Viruses – HSV • Other Factors – smoking, exposure to pesticides • Other Autoimmune diseases – Lupus Erythematosis, pernicious anemia
Clinical Features • 50-60 years • Rapid appearance of vesicles & bullae varying in diameter from a few mm to cm • Rupture of bullae leave a raw, eroded surface • Nikolsky’s sign – loss of epithelium caused by rubbing unaffected skin
Oral Lesions • Range from small vesicles to large bullae • Ill-defined, irregularly shaped, gingival, buccal or palatine erosions, which are painful and slow to heal • Gingival lesions - less common and usually comprise severe desquamative or erosive gingivitis • Soft palate – most commonly involved
Treatment • Topical or intralesional corticosteroids or other immunosuppressants • The treatment of desquamative gingivitis consists of- • Improving the oral hygiene • Minimizing irritation of the lesion • Alternative treatment to corticosteroids – • Chlorambucil, azathioprine, cyclophosphamide • Other drugs – gold, dapsone, prostaglandin E2 • Plasmapheresis • Intravenous immunoglobulins
4. Chronic Ulcerative Stomatitis • It clinically presents with chronic ulcerations and has a predilection for women in their fourth decade of life Oral Lesions • Painful, solitary small blisters and erosions with surrounding erythema are present mainly on the gingiva and the lateral border of the tongue
Treatment • For mild cases - • Topical steroids (fluocinonide and clobetasol propionate) • Topical tetracycline • For severe cases – • Systemic corticosteroids • Hydroxychloroquine sulfate 200 - 400 mg/day
5. Linear IgA Disease (LAD) • Subepidermal vesiculobullous disease that may be idiopathic or drug-induced • Most commonly caused by angiotensin converting enzyme (ACE) inhibitors • Children and adults are affected • Historically known as chronic bullous dermatoses of childhood
Oral Lesions • Vesicles, painful ulcerations or erosions and erosive gingivitis / cheilitis • The hard and soft palates are most commonly affected followed by tonsills, buccal mucosa, tongue and gingiva
Treatment • Combination of sulfones and dapsone • Small amount of prednisone (10-30 mg/day) can be added if the initial response is inadequate • Alternatively, combinations of tetracycline (2 g/day) with nicotinamide (1.5 g/day) have been proved successful
6. Dermatitis Herpetiformis • Rare, benign, chronic, recurrent, immune-mediated blistering dermatologic disease associated with gluten-sensitive enteropathy (GSE) • Approximately 25% of patients with celiac disease have dermatitis herpetiformis • Cutaneous manifestation of celiac disease
Clinical Features • B/W 20 and 55 years • Pruritus and severe burning, followed by the development of erythematous papules, vesicles, bullae or pustules • Extremities, trunk and buttocks – most commonly affected • Vesicles - symmetrical and in groups • Vesicles or pustule eventually resolve and are followed by hyperpigmentation of the skin
Oral Lesions • Vesicles and bullae which rupture rapidly to leave areas of superficial ulceration at any intraoral site
7. Lupus Erythematosus • Autoimmune disease with three different clinical presentations • Systemic lupus erythematosus • Chronic cutaneous lupus erythematosus • Subacute cutaneous lupus erythematosus
Systemic Lupus Erythematosus (SLE) • Etiopathogenesis • Not completely known • Genetics, hormones and the environment (e.g. sunlight, drugs) contribute to disease process • Greater production of autoantibodies immune complex formation and tissue damage
Clinical Features • Peak age of onset - 30 years in females but 40 years in males • Female:male ratio is 10:1 • The cutaneous lesions are characterized by the presence of a rash on the malar area so called butterfly distribution
Oral Lesions • Usually ulcerative or similar to lichen planus • In 36% of patients, oral ulcerations are present • In 4% of patients, hyperkeratotic plaques are present on buccal mucosa and palate
Chronic Cutaneous Lupus Erythematosus (CCLE) • Skin lesions – Discoid Lupus Erythematosus • Oral Lesions • Lichen planus-like plaques on the palate and buccal mucosa • The center of the lesion is slightly depressed and eroded and is covered with a bluish red epithelial surface • On the tongue - circumscribed, smooth, reddened areas in which the papillae are lost or as whitish patches resembling leukoplakia
SubacuteCutaneous Lupus Erythematosus • A group of patients who have a characteristic cutaneous lesion that has similarities to DLE but lacks the development of scarring and atrophy
Treatment • Cutaneous rashes - topical steroids, sunscreens & hydroxychloroquine • For arthritis and mild pleuritis – NSAIDs / hydroxychloroquine • For severe systemic organ involvement - moderate to high doses of prednisone • For severe cases of SLE or when side effects of prednisone develop, immunosuppressive drugs such as cytotoxic agents