Download
1 / 40
400 likes | 415 Views
Learn about gout, a type of inflammatory arthritis triggered by the crystallization of uric acid within the joints. Explore its definition, epidemiology, etiology, pathology, clinical features, diagnosis, and treatment.

E N D
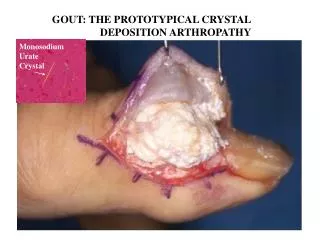
CRYSTAL DEPOSITION DISORDERS BY DR. KAREN D’SA
Thomas Sydenham in 1850 … “ The victim goes to bed and sleeps in good health . About 2 o’clock in the morning he is awakened by a severe pain in the great toe …followed by chills and shivers and …fever The pain which was at first moderate , becomes more intense …so exquisite and lively …in the part affected , that it cannot bear the weight of the bed , clothes nor the jar of a person walking in the room .The night is passed in torture , sleeplessness and a perpetual change of posture …”
INDEX CRYSTALLINE ARTHROPATHIES • GOUT • PSEUDOGOUT • ALKAPTONURIC ARTHRITIS • HYDROXYAPATITE ARTHROPATHY
GOUT • Definition • Epidemiology • Etiology • Pathology • Clinical Features • Diagnosis • Treatment
DEFINITION Hereditary condition of disturbed uric acid metabolism in which monosodium urate crystals are deposited in articular , periarticular and subcutaneous tissues OR Type of inflammatory arthritis that is triggered by the crystallization of uric acid within the joints and is often associated with Hyperuricemia , above 7 mg/dl
EPIDEMIOLOGY • Heredity..occurs in families but not sex linked • Sex : Adult men…females : post menopausal • Male : Female : 8:1 • Consumption of alcohol • High protein diet …red meat and ….also includes seafood
ETIOLOGY • Uric acid is the product of metabolism of purines derived from the diet • 2/3 rds of the uric acid formed each day is excreted in the urine and the rest via the bowel • The concentration of uric acid in the serum depends on the balance between synthesis and excretion
In patients with gout there is impairment of fractional urate clearance via the kidneys usually with normal creatinine clearance • Causes for Hyperuricemia : 1.PRPP SYNTHETase enzyme over activity 2. PRPP SYNTHETASE enzyme RESISTANCE to negative feedback inhibition 3.HGPRTase deficiency 4.GLUCOSE -6- PHOSPHATase deficiency
Purine nucleotides (AMP , GMP) consist of a nitrogenous base (adenosine , guanosine ) , pentose sugar (ribose) and phosphate • Purines are built upon a pre-existing ribose -5 – phosphate • The parent purine nucleotide –inosinemonophosphate is synthesised after a series of reactions adding N and C atoms to ribose 5 phosphate • The first two reactions are rate limiting : conversion of ribose 5 phosphate to phosphoryl pyrophosphate (PRPP) in the presence of PRPP synthetase enzyme. And secondly conversion of PRPP to 5-phosphoribosylamine by PRPP glutamylamidotransferase enzyme. This enzyme is controlled by feedback inhibition of nucelotides ( AMP , GMP , IMP ) • Inosine phosphate is then converted into other purine nucleotides
Free purines formed in normal turnover of nucleic acid are also converted into corresponding nucleotides and this process is known as “Salvage pathway” . • Enzyme Hypoxanthine –guanine phosphoribosyltransferase converts guanine and hypoxanthine to GMP and IMP respectively .Absence of this exzyme produces Lesch-Nyhan Syndrome . • Break down of nucleotides AMP , GMP , IMP are converted to their nucleoside forms (adenosine, inosine , guanosine ) by action of nucleotidase
Inosine and guanosine are respectively converted into hypoxanthine and guanine by purine nucleoside phosphorylase • Adenosine is converted into hypoxanthine and guanine undergoes deamination to xanthine • Hypoxanthine is converted into xanthine by enzyme xanthineoxidase. This enzyme also converts xanthine to uric acid .
At physiological ph and temperature , uric acid is found in a more soluble form as monosodium urate and 7mg/dl is the limit of solubility • At levels above this , it gets deposited in the soft tissues and are called as TOPHI • At 30 degrees , the solubility of Uric acid is lowered further to 4.5mg/dl and is deposited in cooler areas of the body , in the distal joints of the foot • Monosodium urate crystals cause inflammation of the joint by their interaction with neutrophils resulting in release of lysosomal enzymes . Phagocytosisof the crystals by neutrophils causes release of crystal induced chemotactic factor which contribute to inflammation.
1.PRPP SYNTHETase enzyme over activity The enzyme is not subject to normal allosteric controls and leads to increased production of PRPP
2. PRPP SYNTHETASE enzyme RESISTANCE to negative feedback inhibition The abnormal enzyme is active but not sensitive to feedback regulation by inhibitory nucleotides
3.HGPRTase deficiency Leads to increased synthesis of Purine nucleotides
4.GLUCOSE -6- PHOSPHATase deficiency Leads to elevated levels of Ribose 5-Phosphate and PRPP and ultimately purine overproduction
Monosodium urate is deposited as crystals on the surface of articular cartilage .The articular cartilage is eroded and the subchondral bone is replaced in well circumscribed “punched out areas by the crystalline deposits” • Pannus of granulation tissue grows over the articular surface , invades and replaces the articular cartilage and may bridge the joint to the opposite articular surface , producing a fibrous ankylosis • Irregularity of the joint surfaces leads to secondary degenerative arthritis
TOPHI • The tophi are firm , yellow in colour and occasionally discharge a chalky material . • Tophaceous nodules consist of multicentric deposition of urate crystals and intercellular matrix and foreign body granulomatous reaction • As they enlarge in size , calcify , or ossify they can cause pressure symptoms • Nerve tissue is resistant to invasion • Bursa may become distended that the overlying skin is thinned and penetrated resulting in a draining sinus
TOPHACEOUS DEPOSITS 1. Helix of the ear . 2.Antihelix of the ear 3.Fingers 4.Knees 5.Feet 6.Along ulnar surface of forearm 7.Saccular distension of olecranon bursa 8.Subcutaneously along tibial surface
1. UrateNephropathy : • Due to the deposition of sodium urate crystals in the renal interstitial tissue and the resulting inflammatory reaction • This condition is associated with chronic Hyperuricaemia • Manifestations are: Albuminuria • Inability to generate concentrated urine • As the renal disease progresses , azotemia appears and renal failure with acidosis may ensue • Deposits of crystals are seen in the interstitium of medulla with surrounding giant cell reaction
2. Uric acid Nephropathy : • Due to the formation of uric acid crystals in the collecting tubules , pelvis or ureter and the resulting blockade of urine flow • Condition related to Hyperuricaciduria • Hyperuricaciduria is of two types : 1. acute uric acid nephropathy 2.uric acid stones
INVESTIGATIONS • Laboratory findings : SERUM URIC ACID …Normal is <5mg /100ml Microscopic examination of joint fluid : under polarising light microscopy for crystals of monosodium urate ; needle shaped and show strong “negative bi-refringence” Murexide test : few drops of nitric acid + suspected substance ------mixture evaporated to dryness -----moistened with ammonium hydroxide …presence of uric acid -PURPLE COLOUR
X-RAYS : early in the disease – no abnormality • Repeated attacks –joints show erosive changes . Lesions are punched out , sharply marginated lucent pockets with overhanging margins
TREATMENT -CONSERVATIVE • Weight control • Diet restrictions : avoid red meat , alcohol • Ice packs –reduce pain • NSAIDS: • INDOMETHACIN-25 mg/day , may take 12-24 hours • COLCHICINE - inhibits granulocyte migration into the joint -0.5 -1mg/ day • STEROIDS - PREDNISOLONE 40-60mg per day
TREATMENT CHRONIC GOUT : • Febuxostat –non purine selective inhibitor of Xanthineoxidase –dose of 80-120mg • Allopurinol: drug of choice in patients with severe tophaceous deposits and uric acid nephropathy:300mg per day • Uricosuric drugs : decrease serum uric acid by increasing the renal excretion : PROBENECID ( 1-2g/day) & SULFINPYRAZONE
TREATMENT - SURGICAL • Immobilization of the joint will lessen the degree of joint destruction during an acute attack • Tenosynovectomy • Tendon repair or transfer
PSEUDO GOUT • Definition • Epidemiology • Clinical features • Investigations • Diagnosis • Treatment
DEFINITION • Deposition of “Calcium Pyrophosphate Dihydrate” crystals in the joint • Calcium deposits in articular cartilage
EPIDEMIOLOGY • Occurs in persons of either sex , usually over the age of 50 • Classified into 3 groups : 1. Hereditary type 2. CPDD associated with metabolic diseases 3. Idiopathic CPDD
INVESTIGATIONS • Levels of inorganic pyrophosphate are elevated in the synovial fluid • Initial site of crystal formation is articular cartilage • Microscopic examination of synovial fluid : Large number of polymorphonuclear leukocytes Crystals appear as short blunt rods , “Weakly positively birefringent” when seen under polarized light microscope
INVESTIGATIONS • Xray : calcifications in particular hyaline cartilage appear as fine linear densities parallel to and separated from the underlying subchondral bone surface • Calcifications of fibrocartilage appear as thick and irregular densities within the central portion of the joint cavity
TREATMENT • Indomethacin 75-150mg /day for about 10-14 days • Aspiration of synovial fluid followed by intraarticular injection of glucocorticoids