Download
1 / 59
670 likes | 1.42k Views
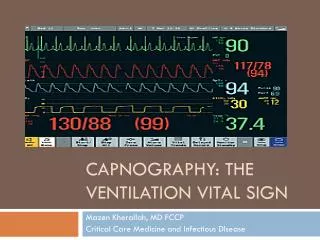
ETCO2 The Vital Sign of Breathing. Jeff Schultz NREMT-P, CCEMT-P Mayo Clinic Medical Transport. EtCO2. Objectives Explain why we measure EtCO2 Distinguish ventilation from respiration Define what is a normal EtCO2 value Define what are abnormal values Identify the different wave forms

E N D
ETCO2The Vital Sign of Breathing Jeff Schultz NREMT-P, CCEMT-P Mayo Clinic Medical Transport
EtCO2 • Objectives • Explain why we measure EtCO2 • Distinguish ventilation from respiration • Define what is a normal EtCO2 value • Define what are abnormal values • Identify the different wave forms • Discuss how to use the sidestream EtCO2 on the Zoll monitor
EtCO2 • Why do we measure EtCO2 • Standard of care • Gives us a measurement of respiratory status • Use as a tool to provide good pt. care
Who Do We Monitor? • Patients with Altered Consciousness • Respiratory distress patients • Overdoses – Drugs and/or ETOH • All intubated patients • Anyone given conscious sedation • Any pt. given pain medications • Any pt. given sedation
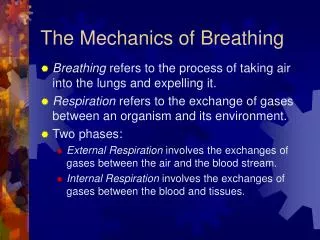
Ventilation vs Respiration • Ventilation is air going in and out • Respiration is the exchange of gases that occur as a result of ventilation, circulation, and metabolism
Capnography Depicts Respiration Metabolism Transport CO2 CO2 O2 CO2 Capnography Ventilation
EtCO2 • What values are normal? • Normal EtCO2 is 30-43mmHg • CO2 can affect pH
EtCO2 • Abnormal Values • EtCO2 of 43 or greater may indicate Respiratory Acidosis • EtCO2 of 30 or less may indicate Respiratory Alkalosis
EtCO2 • Normal values • Normal Range 7.35 to 7.45 • Normal EtCO2 is 30-43mmHg • Normal PaCO2 is 35-45mmHg
EtCO2 • Abnormal Values • Acidosis • pH < 7.35 • PaCO2 > 45 • EtCO2 > 43 • Alkalosis • pH > 7.45 • PaCO2 < 35 • EtCO2 < 30
Where Should We Be? • Our goal is to keep EtCO2 in normal range • Keep EtCO2 30-43 mmHg • Recognize abnormalities in breathing patients • Correct abnormalities in ventilated patients
EtCO2 • How do we stabilize abnormal EtCO2 values? • By adjusting rates • Giving more ventilations • Giving less ventilations
EtCO2 • Stabilizing abnormal EtCO2 values • By Adjusting tidal volumes • Giving less tidal volume • Giving more tidal volume
EtCO2 • Stabilizing Abnormal values • EtCO2 greater than 43mmHg • Increase tidal volume • Increase respiratory rate and/or • This will bring down EtCO2
EtCO2 • Stabilizing abnormal values • EtCO2 less than 30mmHg • Decrease respiratory rate and/or • Decrease tidal volume • This will increase EtCO2
EtCO2 • Identifying the wave forms • Normal wave forms vs. Abnormal wave forms
EtCO2 • Identifying wave forms • Normal wave forms
50 25 0 Beginning of expiration = anatomical deadspace with no measurable CO2 Normal Capnogram - Phase I CO2 mmHg B A
Anatomical Dead Space Anatomical Deadspace Conducting Airway - No Gas Exchange • Anatomical Dead Space • Internal volume of the upper airways • Nose • Pharynx • Trachea • Bronchi Jan Stepanek, M.D., M.P.H.
50 25 0 Normal Capnogram - Phase II CO2 mmHg C exhalation B Mixed CO2, rapid rise in CO2 concentration
50 Alveolar Plateau, all exhaled gas took part in gas exchange 25 inspiration End Tidal CO2 value 0 Normal Capnogram - Phase III CO2 mmHg D C Time
Alveolar Plateau established No Alveolar Plateau Capnogram – Valuable Tool CO2 (mmHg) 50 25 0
EtCO2 • Identifying wave forms • Abnormal wave forms
Capnography Endotracheal Tube in Esophagus • Possible Causes: • Missed intubation • When the ET tube is in the esophagus, little or no CO2 is present • A normal capnogram is the best indication of proper ET tube placement
Capnography Obstruction in Airway or Breathing Circuit • Possible Causes: • Partially kinked or narrowed artificial airway • Presence of foreign body in the airway • Obstruction in expiratory limb of breathing circuit • Bronchospasm
Capnography Muscle Relaxants (curare cleft) • Possible Causes: • Patient attempts to take a breath • Appears when muscle relaxants begin to subside • Depth of cleft is inversely proportional to degree of drug activity
Capnography Cardiac Oscillations • Characteristics: • Rhythmic and synchronized to heart rate
Capnography Inadequate Seal Around ET Tube • Possible Causes: • Leaky or uncuffed endotracheal or trach tube • Artificial airway that is too small for patient
Capnography Hypoventilation - Increase in ETCO2 • Possible Causes: • Decrease in respiratory rate • Decrease in tidal volume • Increase in metabolic rate • Rapid rise in body temperature
Capnography Hyperventilation - Decrease in ETCO2 • Possible Causes: • Increase in respiratory rate • Increase in tidal volume • Decrease in metabolic rate • Fall in body temperature
Capnography Rebreathing • Possible Causes: • Expiratory filter that is saturated or clogged, expiratory valve that is sticking • Inadequate inspiratory flow, or insufficient expiratory time • Anything that causes resistance to expired flow
EtCO2 • Identifying wave forms • Normal vs. abnormal • Case studies
Case Study Normal capnogram, stable trend ETCO2/PaCO2 gradient 4 mmHg
Case Study • Sudden decrease in ETCO2 from 38 mmHg to 20 mmHg and remains there RR increases to 24 bpm
Case Study • Pt. receives 5mg MS for pain and 12.5mg Promethazine for subsequent nausea. • EtCO2 climbs from 37 mmHg to 45 mmHg
EtCO2 • Special Considerations • EtCO2 with RSI and Head Injuries • Standard of care is to keep EtCO2 levels at 32-36mmHg for RSI and head injured patients.
What can ETCO2 monitoring do for you? • Provide “Tube Vigilance” during intubation and transport • Identifies ROSC during CPR • Monitors the breathing status of the obtunded or sedated patient • Tracks progression of acute respiratory failure • For use in a wide range of environments
Your patients are ENVIRONMENTS
Metabolism Pain Hyperthermia Malignant hyperthermia Shivering Circulatory System Increased cardiac output - with constant ventilation Respiratory System Respiratory insufficiency Respiratory depression Obstructive lung disease Equipment Defective exhalation valve Causes of an Elevated ETCO2
Metabolism Overdose / sedation Hypothermia Circulatory System Cardiac arrest Embolism Sudden hypovolemia or hypotension Respiratory System Alveolar hyperventilation Bronchospasm Mucus plugging Equipment Leak in airway system Partial airway obstruction ETT in hypopharynx Causes of a Decreased EtCO2
Sidestream EtCO2 for Zoll • Equipment includes : • LoFlo® module • LoFlo® sampling cannula • Loflo® airway adapter kit
LoFlo® module Clear tube must remain unobstructed
Sidestream EtCO2 Setup • Attach sampling cell to module • Ensure that exhaust tube vents gasses away from module • Turn Zoll monitor on • “Warm Up” will be displayed • Unit will give readings while warming up but will not be accurate until warm up is complete
Zeroing the LoFlo® Module • Zeroing should only need to be done once if same module is used with the same Zoll monitor. • Zeroing cannot be done when sampling kit is attached to the patient. • Do not attempt zeroing for 20 seconds after removing the adapter or cannula from the patient’s airway
Select the Appropriate Sampling Kit • There are two types of sampling kits • Nasal cannula sampling kit • Airway adapter sampling kit
Applying the Nasal Cannula Sampling Kit • Apply sampling kit just like any other nasal cannula • Trim oral portion of the cannula to proper length • Tip should be just below the teeth at the mouth • Trim with trauma shears while not on the patient