Download
1 / 30
480 likes | 1.34k Views
Lecture 2 Measurement of Obesity. Bonnie Beezhold, PhD, CHES Assistant Professor, Nutrition Benedictine University. Measurement of body mass index (BMI). BMI correlates significantly with morbidity and mortality

E N D
Lecture 2Measurement of Obesity Bonnie Beezhold, PhD, CHES Assistant Professor, Nutrition Benedictine University
Measurement of body mass index (BMI) • BMI correlates significantly with morbidity and mortality • BMI replaced Met Life height/weight tables and is now important for clinical standards and population comparisons • There is a good correlation between BMI and percent (%) body fat, but not in all ethnic groups
BMI is the ratio of a person’s weight to the square of their height • May be an overestimate in people with high muscle mass (athletes and lactating women) • BMI has the same cut off points for males and females • Women have the same relative risk but lower absolute risk associated with overweight than men, thus women may tolerate body fat better than men cdc.gov
Interpretation of BMI NHLBI Clinical Guidelines on the Identification, Evaluation and Treatment of Overweight and Obesity in Adults-the Evidence Report. Obesity Research 1998:(suppl.) 53S.
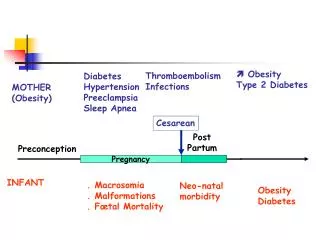
Measurement of obesity - body fat Distribution People store body fat in two general ways, around the middle or around the hips/buttocks/upper legs The “apple shape” fat distribution predicts levels of cardiovascular risk factors and disease Shape of most men and postmenopausal women
How to measure body fat distribution Waist circumference and waist-to-hip ratio Waist circumference is the simplest and preferred way Predicts intra-abdominal fat as accurately as WHR Correlates strongly with intra-abdominal adipose tissue as assessed by a CT scan or MRI
Do WC values apply to all? Ethnic-specific values for waist circumference (adapted from the IDF consensus worldwide definition of the metabolic syndrome, available at http://www.idf.org) Country/Ethnic group Waist circumference Europids (in USA, the ATPIII values Male 94 cm are likely to be used in clinical practice) Female 80 cm South Asians Male 90 cm Female 80 cm Japanese Male 85 cm Female 90 cm East Mediterranean and Middle East Male, use European cut-off Population values until more specific data are available
Body composition • Humans are assumed to have a body composition consisting of 80% lipid, 14% water, 5% protein, and <1% mineral • Most important consideration in evaluating body weight and composition is the proportion of total body weight that is fat (% body fat) • Body fat is the most variable constituent of the body; consists of essential fat and storage fat
Essential fat • Fat stored in bone marrow, heart, lungs, liver, spleen, kidneys, intestines, muscles, and lipid-rich tissues throughout the central nervous system • Required for normal physiological functions • Reducing essential fat below some minimal amount can impair overall health • Extremes in dieting (and exercise) can reduce essential fat stores
Storage fat (adipose tissue) • Located around internal organs (visceral fat) and directly beneath the skin (subcutaneous fat) • Provides bodily protection, serves as an insulator, energy reservoir • Level of adiposity, age, gender, heredity all play an important role in determining AT composition
Body composition changes over time The relationship between subcutaneous fat and internal fat may not be the same for all individuals and may fluctuate during the life cycle. People get fatter when they get older even when their body weights are stable.
Body fat development Three times in life we develop or form fat cells: 3rd trimester in utero first year of life puberty Fat cells may change size, but they will not “burn off”…so, by exercising in the “fat burning” zone, we are actually reducing the size of fat cells
Most people, no matter the size, have around 75 billion fat cells
How much body fat is too much? Too much body fat can have negative physiologic effects Once men exceed 25% and women 32% fat, there is a dramatic correlation with illness and disease Dyslipidaemia, impaired heart function, heart disease and hypertension, cancer, impaired immunity, gallbladder disease, kidney disease, insomnia/apnea, skin problems
Measurement of body composition Atomic, molecular, cellular, tissue, whole body levels Methods range from simple to complex with all having limitations and some degree of error 2-component (2-C) model partitions body into fat mass (FM) and fat-free mass (FFM) 3-C model partitions body into FFM, FM, and total body water(TBW) 4-C model includes FM, TBW, and components of FFM (minerals, total body protein) The more components measured, the more difficult and costly the measurements are to perform, but fewer assumptions required.
Fat-free mass (FFM) • Devoid of all extractable fat; ‘dry’, containing mainly protein and minerals • Determinant of metabolic rate (BMR, RMR) • Composed of metabolically active body mass such as organs and muscle mass • Brain, heart liver and kidney have greater rates • Also composed of supporting tissue such as bone and fluid
Laboratory methods: most common are 2-C methods of densitometry and hydrometry Field methods: most common are skinfold thickness and bio-impedance analysis (BIA) Methods are often used with prediction equations to estimate components at the other four body composition levels Whole body measurement (level V)
Triceps: • Vertical fold • Posterior midline of the upper arm • Halfway between acromion (shoulder) and olecranon processes (elbow) • Arm held freely to side of body • Subscapula: • Diagonal fold • 1 to 2 cm below the inferior angle of the scapula • Suprailiac: • Diagonal fold • Anterior axillary line (modern technique) • immediately superior to iliac crest • in line with natural angle of iliac crest • Mid-axillary line (traditional technique) • Superior to iliac crest Usually the subscapular and triceps are measured
Energy balance • Energy intake – equal to the energy liberated during the oxidation of food • Energy expenditure – includes the energy: • immediately lost as heat (thermogenesis) • used to do work (driven by ATP) • stored in C-C and C-H bonds and… • In liver and muscles as glycogen • In adipose tissue as triglycerides • In body protein (~50% available for energy if needed)
Types of thermogenesis Isothermic thermogenesis: due to changes in muscle tone without any work done Dynamic thermogenesis: from stretched muscle without any work Psychological thermogenesis: anxiety, stress stimulate epinephrine secretion Cold-induced thermogenesis: thermal regulation; shivering vs non-shivering Diet-induced thermogenesis: following a meal Drug-induced thermogenesis: caffeine (60-80mg raises BMR 5-10% over 1-2 hrs), nicotine, alcohol Miller ,1982
Components of Daily Energy Expenditure Segal KR et al. Am J Clin Nutr. 1984;40:995-1000.
Alternative compartmentalization of energy expenditure • Based on resting and non-resting metabolic rate • Involuntary activity (fidgeting) is always referred to as non-exercise activity thermogenesis (NEAT) ) Dulloo & Jacquet, 2003
Estimating energy requirements (kilocalories) • Energy requirements are related to energy expenditure (EE) which depends on body size and composition • Assessing body composition vs just body weight is more accurate to find true requirements, however, body composition varies • Estimates of energy requirements are based on BMR multiplied by a PA factor • Accuracy of estimate would be improved by using FFM, but assessing FFM is not available on a population level
Metabolic rate 25 • Basal metabolic rate (BMR) reflects the energy required to perform the most essential activities • Largest determinant is body size (particularly FFM); rate declines by 1-2% per decade between ages 20-70 (declining FFM) • Resting metabolic rate (RMR) reflects resting energy expenditure (REE) occurring during normal cellular and organ functions • Total metabolic rate (TMR) is the total rate of kilocalorie consumption to fuel all ongoing activities
How do we measure metabolic rate? • Direct calorimetry - measurement of the amount of heat produced by a subject enclosed within a small chamber - most accurate • Indirect calorimetry - measures gas exchange after resting - accurate to within 5% http://www.letmedical.com/products
How do we estimate RMR?Predictive equations are population specific Harris-Benedict equation - most widely used Mifflin's equation - estimates RMR to within 10% of that measured (Frankenfield et al, 2005) Cunningham's equation - more appropriate for athletes http://www.exercisebiology.com/
Energy expenditure due to Physical Activity 29 Amount expended depends on type, intensity, frequency of PA Contribution: 10-15% Measurement: characterized at different levels of effort based on the standard of a metabolic equivalent (MET), the unit used to estimate the amount of oxygen used by the body during PA (Ainsworth et al., 1993)
Discrepancy Between Reported and Actual Energy Intake and Expenditure