Download
1 / 11
110 likes | 386 Views
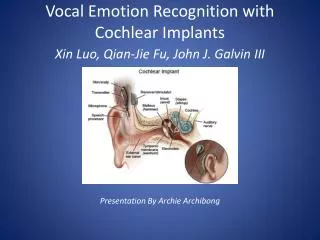
Cochlear Implants and Meningitis: A Case for Collaborative Surveillance. Krista Biernath/Pam Costa 2005 EHDI Conference Atlanta, Georgia March 3, 2005. Background. June 2002, FDA received first reports of bacterial meningitis in cochlear implant recipients.

E N D
Cochlear Implants and Meningitis: A Case for Collaborative Surveillance Krista Biernath/Pam Costa 2005 EHDI Conference Atlanta, Georgia March 3, 2005
Background • June 2002, FDA received first reports of bacterial meningitis in cochlear implant recipients. • Subsequent investigation identified meningitis episodes from 1/1/97 – 9/15/03. • Incidence of meningitis in children with cochlear implants caused by S. Pneumoniae was 30 times higher than general population. • Post-implant meningitis was significantly associated with use of a positioner.
Background (Continued) • Models with the positioner were available from 1999–July 2002. • On-going cases of post-implant bacterial meningitis among cochlear implant users prompted a new investigation. • Need to be vigilant during post-operative period for all and long-term for children with positioners. • Vaccine recommendations apply for all children with cochlear implants. http://www.cdc.gov/nip/recs/child-schedule.htm
The Concern • Ongoing evidence that children with cochlear implants are developing meningitis • Currently, state surveillance of these events is uncoordinated or not occurring • Without accurate data, the potential public health question can not be adequately addressed
Current Status-Infectious Disease Reporting • States differ in what types of meningitis are reportable under their infectious disease requirements: some state comments • “only meningitis cause by Neisseria meningitides and H-Flu” • “bacterial and viral” • “disease specific, including Neisseria, H-Flu, Strep. Pneumoniae, some viral-LaCrosse, West Nile)
Infectious Disease Reporting Cont. • States differ as to what data are collected on infectious reporting forms, with regard to cochlear implants • Most states report cochlear implant status not collected routinely, if at all • 2 years ago, asked “Could forms be changed?” • Yes, no, not easily, probably-if there is evidence that it would be useful
Current Status-EHDI systems • Some EHDI systems are set-up to gather information about device type, including cochlear implants • Unknown if any state EHDI systems currently collecting information about meningitis occurrence • Few EHDI programs have on-going relationships with state infectious disease surveillance
CDC Next Steps • CDC EHDI will continue to be in contact with state epidemiologists • CDC EHDI will be requesting that all states modify their infectious disease reporting forms to include at least two questions: • Is the person deaf/hard of hearing • Does the person have a cochlear implant
State/Territorial Next Steps • Encourage state/territory’s EHDI programs to collaborate with their infectious programs • Learn what is reportable in your state/territory • Determine if data can be shared • Work with audiologists/medical home for other opportunities for reporting-Strep. Pneumoniae not reportable for many states/territories
National Next Steps • CDC EHDI will continue to work with FDA • CDC EHDI will encourage states/territories to report cases (de-identified) to CDC EHDI • Date of birth • Type of meningitis • Perhaps other common variables (?) • Need for continued surveillance to address public health concern
Further Information • CDC-EHDI • http://www.cdc.gov/ncbddd/ehdi/ • Recommended vaccination schedule • http://www.cdc.gov/nip/recs/child-schedule.htm