Download
1 / 19
190 likes | 449 Views
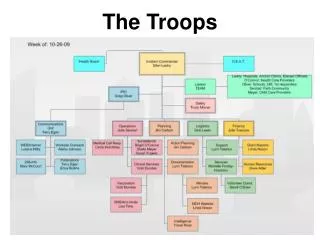
MOVING THE TROOPS THROUGH Enrollment to Randomization. Logistics. 6 Month treatment period Visits at weeks 0, 2, 8, 16 and 26 5 year follow up period 1 year clinic visits 4 year telephone contact Central laboratory: All tests provided Central pharmacy: Aptuit

E N D
Logistics • 6 Month treatment period • Visits at weeks 0, 2, 8, 16 and 26 • 5 year follow up period • 1 year clinic visits • 4 year telephone contact • Central laboratory: All tests provided • Central pharmacy: Aptuit • Paper reports faxed to Core for data entry
Inclusion criteria • Primary FSGS confirmed by renal biopsy or genetic testing • Failure to respond to prior therapy at least one of the following immunosuppressive medications-cyclosporine, tacrolimus, MMF, sirolomus • Age 1-65 years at onset of proteinuria • Estimated GFR ≥40 ml/min/1.73 m2 at screening and ≥30 ml/min/1.73 m2 at randomization
Inclusion criteria • Up/c > 1.0 g/g creatinine on first morning void • Steroid resistance defined as failure to achieve sustained Up/c <1.0 following a standard course of prednisone/prednisolone/methylprednisolone OR contraindication/anticipated intolerance to steroid therapy.
Exclusion criteria • Lactation, pregnancy, or refusal of birth control in women of child‑bearing potential • Participation in another therapeutic trial involving protocol mandated administration of a immunosuppressive medication concurrently or 30 days prior to randomization • Active/serious infection (including, but not limited to hepatitis B or C, HIV) • History of malignancy • Abnormality in age appropriate cancer screening in accord with ACS 2003 guidelines • Uncontrolled BP > 140/95 or > 95th percentile for age/height at the end of the run in period • Diabetes mellitus Type I or II.
Exclusion criteria • Organ transplantation • Congestive heart failure • History of prior myocardial infarction • SLE or multiple sclerosis • Hepatic disease defined as serum AST/ALT >2.5X upper limit of normal • Hematocrit <27% • Immunosuppressive therapy with cyclosporine, Tacrolimus, MMF, azathioprine, rapamycin, or cyclophosphamide in the 30 days prior or Rituximab in the 90 days prior to randomization • Prior treatment with adalimumab or galactose • Allergy to study medications • Abnormal pap smear (more than CIN I)
Screening visit • History and Physical exam • HIV, HEP B/C if not done in the past 12 months • PPD if not done in the past 12 months • All labs to Spectra, with 2 specimens for Up/c • Existing renal biopsy tissue sent to study pathologist to confirm FSGS
Screening visit-key points • Review all CRFs for completion/accuracy • Ensure that the patient has a negative cancer screening according to the ACS 2003 guidelines • Patients should be on target doses of lisinopril and losartan by the end of the screening period (prior to week 0 visit) • Schedule week 0 visit once you have received drug from Aptuit
Abbreviated Screening Period • If a subject is already on medication and has reached target doses of ACEi and ARB for a minimum of 2 weeks at the time of the B01 visit, the B02 visit will not be required. • The B02 visit is held primarily for safety reasons. It is done to ensure that implementation of the combination of ACEi and ARB at the target doses does not cause a decline in GFR below 30 mL/min/1.73 m2, the eligibility cut off. The subject will receive a screening GFR at B01 to ensure that a decline below 30 mL/min/1.73 m2 has not occurred.
Cancer Screening Overview • Age > 21 and female: Annual Pap smear. • Age > 40 and female: Annual Pap smear AND mammogram. • Age > 50: Annual screen for occult fecal blood. • Age > 50 and male: Annual screen for occult fecal blood and PSA Cancer screening is essential because of the use of adalimumab
Medications Adalimumab (Humira) • SQ injection every other week • Dose is 24 mg/m2/dose • Maximum dose 40 mg
Galactose Powder mixed with water administered bid Dose is 0.2g/kg/dose Maximum dose 15 g Medications
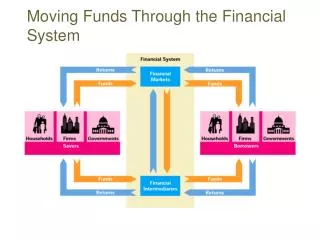
Randomization • Fax all forms to your core site for data entry • Once your patient is randomized you will receive -initial prescription report -drug allocation report • Drug will be shipped to your site from Aptuit within 1-2 business days
Drug Distribution Center(APTUIT) • Drugs provided: Atorvastatin Galactose, Humira • Prescription for: lisinopril and losartan • Drugs will be shipped from Aptuit once patient is randomized
Central Laboratory (Spectra East) • CBL measurements: Urine protein/creatinine, urine pregnancy testing, all serum chemistries, fasting lipid profile, hematology, Screening for HIV, HEP B, and HEP C • Spectra to send kits with Fed Ex labels, shipping boxes, tubes, collection cups, ice packs, etc. • Spectra faxes routine results to PSs, transmits results to central data base overnight. • Immediate “panic reports” of life-threatening values
Visits • All Forms are available on line https://clinicalresearch.ccf.org • Visits should be held within 3 days on either side of target date • Once week 0 visit is entered, a visit schedule will be sent to site
DCC Reports Eligibility (every other day until participant is randomized or considered ineligible) Core Lab (results of urine and or blood/serum samples sent to Spectra) Biopsy Results (sent when Core Pathologist completes/enters F287) AE/SAE (F260, F261 entered; this report will go to NIH Project Officer as well) Reminders (an e-mail stating next visit window and what is expected for that visit) Action Items (BP out-of-range, high or low lab values, etc) DCC e-mail alias is font_dcc@bio.ri.ccf.org
REIMBURSEMENT • $1250 per center start-up • Effort for IRB application and contract • Pharmacy start-up • Administrative fees • Dispersed upon receipt of IRB approval and signed contract with Clinical Coordinating Center • $3375 per patient enrolled