Download
1 / 58
581 likes | 763 Views
Trends, Issues & Treatment in Late-Stage Prostate Cancer. Oliver Sartor, M.D. LaBorde Professor for Cancer Research Medical Director, Tulane Cancer Center Tulane Medical School New Orleans, LA. Charles B. Huggins.

E N D
Trends, Issues & Treatment in Late-Stage Prostate Cancer Oliver Sartor, M.D. LaBorde Professor for Cancer Research Medical Director, Tulane Cancer Center Tulane Medical School New Orleans, LA
Charles B. Huggins • “Despite regressions of great magnitude, it is obvious that there are many failures of endocrine therapy to control the disease.” • Nobel Lecture • December 13, 1966
“Castrate-Refractory” Prostate Cancer • Progressive prostate cancer despite surgical or medical castration • Serum Testosterone (<50 ng/dL)
“Castrate-Refractory” Prostate Cancer: The Face of Change • Many changes have occurred in our understanding of this disease • Pathophysiology • The evolution from “hormone-refractory” and “androgen-independent”, to “castrate-refractory” • Therapeutic options • Current Standards • Multiple new paradigms on the rise
Pathophysiology: The Continued Importance of the Androgen Receptor
Androgen Receptor Gene Over-Expression in “Castrate-Refractory” Prostate Cancer Linja et al., Can Res 61:3550 2001
Tissue Androgen Levels in Benign Prostate vs. Castrated Cancer Tissue Shaded=Benign Clear=Castrate Mohler et al., Clin Cancer Res 10:440, 2004
Over-Expression of Enzymes in the Androgen Synthesis Pathway in Metastatic Castrate-Refractory Prostate Cancer Cells Stanbrough et al. Cancer Res. 66:2815, 2006
Ligand-Independent Androgen Receptor Variants Derived from Splicing of Cryptic Exons Signify CRPCHu et al. Cancer Research 69:16-22, 2009
Conclusions • Androgen receptor signaling remains a key factor in prostate cancer growth despite castrate serum levels of testosterone • The prostate cancer switches from a traditional endocrine paradigm to an autocrine/paracrine paradigm BUT some of the apparent mechanisms of AR activation are ligand-independent
Therapeutic Options for CRPC Today • Secondary Hormonal Manipulations • Antiandrogen Withdrawal, Antiandrogen Administration, Adrenal Suppressives (ketoconazole), Corticosteroids (prednisone, dexamethasone, etc.), Estrogens (DES, etc.) • External Beam Radiation Therapy • Intravenous Bone-seeking Radioisotopes • Samarium-153 EDTMP, Strontium-89 (FDA approvals) • Bisphosphonates • Zoledronate (FDA approval) • Chemotherapy • Mitoxantrone, docetaxel, estramustine, cabazitaxel (FDA approvals) • Immune Therapies • Sipuleucel T (FDA approved) • Experimental Therapies (Clinical Trials)
Despite Many New Promising Agents, Docetaxel was, For Many Years, the only FDA Approved Chemotherapy shown to have a Survival Benefit in CRPC
Phase III Docetaxel Studies in HRPC Demonstrating Survival Benefit Mitoxantrone 12 mg/m2 Prednisone 10 mg q day Q 21 days up to 10 cycles TAX 327 Randomize Docetaxel 30 mg/m2/wk Prednisone 10 mg q day 5 on; 1 off x 6 cycles N=1006 Docetaxel 75 mg/m2 Prednisone 10 mg q day Q 21 days up to 10 cycles SWOG 9916 Mitoxantrone 12 mg/m2 Prednisone 5 mg bid Q 21 days Randomize N=770 Docetaxel 60 mg/m2 d 2 Estramustine 280 mg d1-5* Dexamethasone 20 mg, tid d 1 & 2 *Warfarin and aspirin Tannock et al. N Engl J Med 2004:351;1502-1512; Petrylak et al. N Engl J Med 2004;351:1513-1520.
Overall Survival Petrylak et al. N Engl J Med 2004;351:1513-1520 100% 80% 60% 40% 20% 0% 0 12 24 36 48 Months # at Risk # of Deaths Median in Months D+E 338 217 17.5 M+P 336 235 15.6 HR: 0.80 (95% CI 0.67, 0.97), p = 0.01
Overall Survival: Tax 327Tannock et al. N Engl J Med 2004:351;1502-1512 1.0 Docetaxel 3 wkly 0. 9 Docetaxel wkly 0.8 Mitoxantrone 0.7 0.6 Probabilityof Surviving 0.5 Median survival Hazard (mos) ratio P-value Combined: 18.2 0.83 0.03 D 3 wkly: 18.9 0.76 0.009 D wkly: 17.3 0.91 0.3 Mitoxantrone 16.4 – – 0.4 0.3 0.2 0.1 0.0 0 6 12 18 24 36 Months
New Agents in CRPC Clinical Trials (#1) • Vaccines and immune stimulants • PROSTVAC-VF-Tricom Vaccine (phase III in planning) • Anti-CTLA4 (Ipilimumab phase III underway post-docetaxel) • GMCSF • Angiogenesis inhibitors • Lenalinomide (Revlimid phase III well underway) • Bevacizumab (Avastin phase III negative 3/12/10) • VEGF TRAP (Aflibercept phase III accrual completed) • Novel Anti-Tubular Agents • Cabazitaxel (phase III announced positive 12/09 and FDA approved June 17, 2010!) • Ixabepalone (phase III in combination with mitoxantrone in planning post-docetaxel)
New Agents in CRPC Clinical Trials (#2) • Newer Androgen-Signaling Targeted Therapies • Abiraterone , Cougar phase III post-docetaxel accrual complete in 4/09 and pre-docetaxel accrual completed 5/10) • Takeda and Tokai androgen synthesis now in trials • AR blockade (MDV3100, Sawyers new compound) • MDV3100 phase III underway • Newer Signal Transduction Inhibitors • PI3 Kinase (Exelexis XL147, Novartis BEZ235, Genentech GDC-0941, Semafore SF 1126) • p60src and other kinases (dasatinib phase III well underway) • Multi-kinase inhibitor (sunitinib phase III well underway)
New Agents in CRPC Clinical Trials (#3) • Bone targeted agents • Isotopes: radium-223 (alpharadin phase III well underway) • Isotopes: strontium-89 (phase III underway with taxotere) • RANK ligand: denusomab phase III accrual complete for metastases prevention vs placebo and also vs zoledronic acid for SREs (announced as positive 2/10) • Endothelin antagonists • Atrasentan (failed monotherapy phase III but in docetaxel combination phase III completed accrual 5/10) • ZD4054 (Three phase III trials, one with docetaxel and 2 without (M0 and M+): All but M0 completed accrual
New Agents in CRPC Clinical Trials (#4) • Stem cell targeted agents • Anti-Prostate stem cell antigen (PSCA), • Sonic hedgehog (IPI-926, others) • Prostate specific surface targets • Anti-PSMA (J591, 7E11, MLN2704, others) • New generation of various aptamers and targeted nanoparticles • Chemotherapeutic resistance and apoptotic regulators • Anti-Clusterin (OGX-011 or custirsen) phase IIIs in planning for both chemo-naïve and post-docetaxel • AT-101 (gossypol) phase III in planning
Selected Phase III Trials That Have Completed Accrual in Prostate Cancer • Docetaxel/bevacizumab vs docetaxel in chemo-naïve mCRPC (CALGB) • Announced negative March 12, 2009 • XRP6258 (cabazitaxel) vs mitoxatrone post-docetaxel in mCRPC (Sanofi-Aventis) • Announced positive 12/09, presented 3/10 at ASCO GU, FDA 6/10 • Abiraterone vs prednisone post-docetaxel in mCRPC (Cougar) • Anticipated late 2010 • Denusomab vs placebo in metastases prevention in non-metastatic CRPC • Fall/Winter 2010 anticipated • Denosumab vs zoledronate for SRE prevention in mCRPC • Announced positive 2/9/10 for SRE, presented ASCO 6/10
Selected Novel Therapeutics and Concepts in for CRPC • New hormonal therapies • Abiraterone and MDV3100 • A new chemotherapy • Cabazitaxel • A new immunotherapy • Sipuleucel-T • A brief mention, “Stromal Targeted” therapies
Abiraterone: Potent Inhibitor of CYP17: (17-20 Lyase and 17-Alpha Hydroxylase)
Maximal PSA Declines in Abiraterone Post-DocetaxelReid et al. JCO 28:1489, 2010
MDV3100: A New Anti-AndrogenTran et al: Science 324:787-790, 2009
MDV3100 PSA Changes in Phase I TrialScher et al. ASCO GU, 2009, #151
PSA Declines with MDV3100 Pre- and Post-DocetaxelScher et al. Lancet 375:1437, 2010
Reminder • AR targeted therapy effects PSA disproportionately to tumor volume • PSA gene has an androgen response element in the promoter • Effects on survival with the new AR targeted therapies are yet to be reported
Cabazitaxel:A New Tubulin-Targeting Agent • New semi-synthetic taxane • Selected to overcome the emergence of taxane resistance¹,² • Preclinical data¹,² • As potent as docetaxel against sensitive cell lines and tumor models • Active against tumor cells/models resistant to currently available taxanes • Clinical data • Antitumor activity in mCRPC including docetaxel-resistant disease³ 1. Attard G, Greystoke A, Kaye S, De Bono J. Pathol Biol (Paris). 2006;54(2):72-84. 2. Pivot X, Koralewski P, Hidalgo JL, et al. Ann Oncol. 2008;19(9):1547-1552. 3. Mita AC, Denis LJ, Rowinsky EK, de bono JS et al. Clin Can Res. 2009; Jan 15;15(2):723-30.
TROPIC: Phase 3 Study: 146 Sites, 26 CountriesSartor et a. GU ASCO 2010 Hormone Resistant Metastatic Prostate Cancer Patients Previously Treated With A Taxotere Containing Regimen Randomization (1:1) Stratified for Measurability of Disease and ECOG PS cabazitaxel 25 mg/m² q3w + Prednisone* mitoxantrone 12 mg/m² q3w + Prednisone* 755 patients, Maximum treatment duration 10 cycles, planned 511 events to detect 25% reductionin hazard ratio, 90% power, 2 sided 5% alpha level Primary endpoint = Overall Survival, Secondary endpoint = PFS, response rate and safety, interim (futility) PFS based analysis after 225 events * Or prednisolone – 10 mg given orally daily
Eligibility Criteria • mCRPC patients with documented disease progression • If measureable: RECIST progression • If non-measurable : Documented rising PSA levels (at least2 consecutive rises in PSA over a reference value taken at least 1 week apart ) or appearance of new lesion • Previous treatment with at least 225 mg/m2 docetaxel-containing regimen (protocol amended) • No previous treatment with mitoxantrone • ECOG-PS: 0–2 • Normal organ function (CBC and serum chemistries) • No grade 2 or worse neuropathies
100 MP CBZP Median OS 0.70 Hazard Ratio 80 95% CI 0.59–0.83 <.0001 P-value 60 40 20 0 6 months 12 months 18 months 24 months 30 months 0 months Primary Endpoint: Overall Survival (ITT Analysis) Proportionof OS (%) 12 .7 15.1 Numberat risk Sartor et al. GU ASCO, 2010
0 1 2 Hazard Ratio Subgroup Overall Survival Analysis Favors CBZ
0 1 2 3 Hazard Ratio Subgroup Overall Survival Analysis Favors CBZ
100 80 60 40 Censored MP 20 CBZP Combined medianfollow-up: 13.7 months 0 0 3 6 9 12 15 18 21 Time (months) Numberat Risk MP CBZP Progression-Free Survival 25% reduction in risk of progression Proportion of PFS (%) 377 378 117 168 55 92 30 55 12 18 9 6 6 1 4 1
Secondary Endpoints:Response Rate and Time to Progression *Determined only for subjects with at baseline measurable disease, PSA ≥20 ng/ml, or pain, respectively. NR=Not reached.
Most Frequent Treatment-EmergentAdverse Events* *Sorted by ≥2% incidence rate for grade ≥3 events in the cabazitaxel arm.
Hematological Results *Prophylactic use of G-CSF was permitted except for cycle 1 of treatment at the discretion of the investigator. 58% grade ≥3 neutropenia in MP arm of the TROPIC study compares to 22% reported for the TAX 327 (first-line) study
FDA Package Insert on Growth Factors • Primary prophylaxis with G-CSF should be considered for pts >65 years, poor performance status, prior febrile neutropenia, poor nutritional status, or other serious co-morbidities
Cabazitaxel Conclusion • An effective drug fulfilling an unmet need with a safety profile that demands meticulous attention to detail in particular with careful management of neutropenia and diarrhea • It should be reserved for patients with metastatic CRPC with progressive disease post-docetaxel and a good performance status and organ function
7 - IL-3 IL-4 IL-6 IL-2 IL-5 MIF SCF CD2 B7-1 IL IL-10 IFN- TNF- MIP-1 G-CSF IL-1RA MIP-1 M-CSF ICAM-1 GM-CSF IL-2 + IL-1 GM-CSF Induces the Greatest Anti-Tumor Immunity in Cytokine Transduced Tumor CellsDranoff et al, PNAS 90:3539, 1993 100 80 60 % Tumor Free Animals 40 20 0
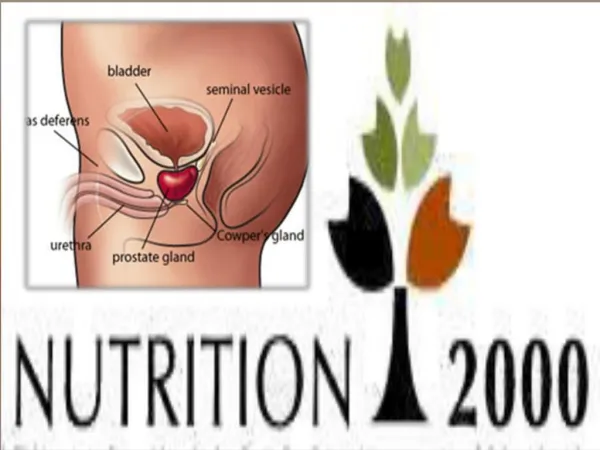
Antigen Delivery Fusion Protein Used to Stimulate Antigen Presenting Cells (APCs) in Preparation of Sipuleucel-T Prostatic Acid Phosphatase (PAP) Granulocyte Macrophase Colony Stimulating Factor (GM-CSF)
Leukapheresis PAP-GM-CSF “Antigen” Isolation of APC Patient Antigen-loaded APCs Vaccination with Antigen (GM-CSF/PAP) Loaded Antigen Presenting Cells (APCs)
Randomized Phase III Trial with Sipuleucel-T (IMPACT or D9902B) S U R V I V A L P R O G R E S S I O N Treated at Physician discretion Sipuleucel-T Q 2 weeks x 3 Asymptomatic or Minimally Symptomatic Metastatic Castrate Resistant Prostate Cancer (N=512) 2:1 Treated at Physician discretion and/or Salvage Protocol Placebo Q 2 weeks x 3 Primary endpoint: Overall Survival Secondary endpoint: Time to Objective Disease Progression
Sipuleucel T: IMPACT Phase III Trial Overall Survival Provenge (n = 341) Median Survival: 25.8 Mos. Placebo (n = 171) Median Survival: 21.7 Mos. P = 0.032 (Cox model) HR = 0.775 [95% CI: 0.614, 0.979] Median Survival Benefit = 4.1 Mos.