Download
1 / 24
240 likes | 389 Views
Statistical Review of Intergel. by Richard Kotz Statistician, CDRH/OSB. Outline. Part I: Original Study Protocol and Results Sponsor’s Proposed Sample Size Sponsor’s Proposed Protocol/Analysis Plan Issue of Pooling Data Across Continents Stratified Study Results

E N D
Statistical Review of Intergel by Richard Kotz Statistician, CDRH/OSB
Outline • Part I: Original Study Protocol and Results • Sponsor’s Proposed Sample Size • Sponsor’s Proposed Protocol/Analysis Plan • Issue of Pooling Data Across Continents • Stratified Study Results • Part II: Sponsor’s Revised Claim • Review of Secondary Endpoints • Review of post-hoc endpoint: AFS scores • Summary
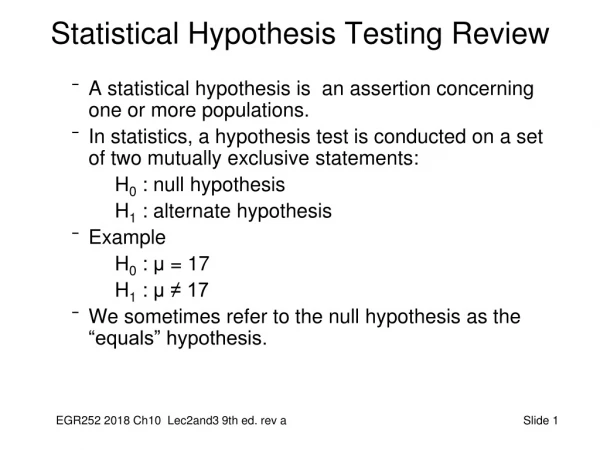
Part I. Original Study Protocol, Design, and Results • Study designed to evaluate whether Intergel in superior to a Control (Lactated Ringer’s) with respect to reduction in adhesion score • Primary Endpoint: Modified AFS (mAFS) • Secondary Endpoint: Number of Sites with Adhesions (Number of Adhesions) • Additional Endpoints: Subsets of total adhesions: Reformed, DeNovo, and Surgical Site Adhesions
Sponsor’s Proposed Sample Size 1. From Pilot Study of Size 20 Observed Difference in mAFS score = 4.0 Intergel = 1.7 (s.d.= 1.4); Control = 5.7 (s.d.= 2.8) 2. Expected Loss to Follow-up (LF) a. Assumed 20% for Intergel; 10% for Control b. give LF worst mAFS score (16.0) 3. Now Effect Size for mAFS scores = 2.1 s.d. = 5.0, Power =80%, Alpha = 5% (2-sided) 4. Sample Size necessary = 90 subjects/arm
Sponsor’s Proposed Protocoland Analysis Plan • 200 U.S. Subjects To Be Enrolled • Unless 120 U.S. and 80 European combinable • Intent-to-Treat (ITT) Analysis • assign worst scores to subjects lost to follow-up • Nonparametric Statistics • mAFS scores very skewed to right • Wilcoxon Rank-Sum Test
Pooling: Conditions for Pooling Data Across Continents • The sponsor specified 3 conditions in the protocol which must be satisfied in order for patients to be combined across continents: 1. Baseline demographic/pre-treatment variables (including adhesion scores) should be similar. 2. There should be no significant interaction between continent and treatment efficacy. 3. Second look scores should be similar. • If not combinable, only US data to be used.
Pooling: Comparison of Baseline Adhesion Scores by Continent U.S.Europep* Intergeln=102 n=41 mAFS 0.781.57 <.01 # Adhesions 2.496.00 <.0001 Controln=98 n=40 mAFS 0.681.95 <.0001 # Adhesions 2.276.40 <.0001 * 2-sample t-test
Pooling: Comparison of Change in mAFS from Baseline Results by Continent Intergel USEurope Sample size n=102n=41 Baseline 0.781.57 2nd Look* 2.63 2.01 Difference 1.85 0.44 * Unadjusted (for adhesions unlysed at baseline) mAFS 3 U.S. 2 EUROPE 1 Baseline 2nd Look
Pooling: Comparison of Change in mAFS from Baseline Results by Continent Control USEurope Sample size n=98n=40 Baseline 0.681.95 2nd Look* 2.76 2.12 Difference 2.0 0.17 * Unadjusted (for adhesions unlysed at baseline) mAFS 3 U.S. 2 EUROPE 1 Baseline 2nd Look
Pooling: Comparison of Change in Number of Adhesions from Baseline by Continent Intergel USEurope Sample size n=102n=41 Baseline 2.496.00 2nd Look* 8.29 7.37 Difference 5.80 1.37 * Unadjusted (for adhesions unlysed at baseline) Adhesions 9 U.S. EUROPE 6 3 Baseline 2nd Look
Pooling: Comparison of Change in Number of Adhesions from Baseline by Continent Control USEurope Sample size n=98n=40 Baseline 2.276.40 2nd Look* 8.07 8.20 Difference 5.80 1.80 * Unadjusted (for adhesions unlysed at baseline) Adhesions 9 EUROPE U.S. 6 3 Baseline 2nd Look
Pooling: Subjects cannot be Pooled across Continents • Baseline values statistically different: mAFS and # adhesions 2 to 3 times > in Europe • Interaction between change from baseline and continent: At 2nd look, US is 3-4 times greater than baseline while Europe is only 10% to 30% greater • Therefore, not appropriate to pool data and U.S. data set represents appropriate data set to evaluate.
Effectiveness of Intergel • Is Intergel solution more effective than Lactated Ringer’s in reducing number of post-surgical adhesions? • Effectiveness evaluated by the primary endpoint (mAFS) and secondary endpoint (number of adhesions) • Appropriate Statistical Analysis Group: All 200 U.S. patients
U.S. ITT Results for mAFS and Number of Adhesions Intergel* Control*Difference** mAFSn=102 n=98 Baseline 0.78 0.68 +0.10 2nd Look* 2.74 2.83 -0.09 Adhesions Baseline 2.49 2.27 +0.22 2nd Look* 8.29 8.07 +0.12 * Unadjusted for adhesions unlysed at baseline **All differences were non-significant (Wilcoxon test)
Are Intergel and the Control Different for the mAFS and Number of Adhesions? • When using appropriate analysis (US, ITT): 1) No statistically significant difference between Intergel and the Control for mAFS score 2) No statistical significant difference between Intergel and the Control in number of adhesions
Conclusion: mAFS and Adhesion Data • Data are not combinable across continents • There is not a statistically significant difference between the Intergel patients and the control patients with respect to mAFS score and number of adhesions.
Part II. Post-Panel Amendment: Revised ‘Indication for Use’ • 1st part of revised claim addresses adnexal adhesions: the sponsor uses AFS score (not mAFS) to support claim • 2nd part of revised claim addresses pelvic and abdominal adhesion reformation: sponsor uses selected secondary endpoints (reformed and surgical site adhesions) • All results for these endpoints were presented to previous Panel
Review of Secondary Endpoints • Failed to detect difference in mAFS or total number of adhesions, therefore scientific validity of evaluation of selected subsets of the endpoint (total number of adhesions) is questionable • Present US, ITT analysis for secondary endpoints: reformed, denovo, and surgical site adhesions.
Average Number of Adhesions at Second Look for Secondary Endpoints Adhesion TypeIntergel*Control*Diff^ n=102 n=98 Baseline 2.49 2.27 +0.22 Reformed 3.18 3.51 -0.33 Surgical Site 2.29 2.62 -0.33 DeNovo 6.71 6.34 +0.37 * Average # of adhesion sites per patient at 2nd look ^ All p-values on differences non-significant (Wilcoxon test)
No Statistical Difference in Secondary Endpoints • Not only were there no statistical difference between groups for mAFS and Number of Adhesions but there was no statistical difference in any of the secondary endpoints (reformed, denovo, or surgical site adhesions) when using the appropriate ITT analysis of the US patients.
Analysis of AFS Scores • Exploratory analysis on a retrospective endpoint not originally specified in protocol • Sponsor analyzes evaluable patients combined across continents (not the appropriate ITT, US data) • Appropriate presentation of data: ITT, US
AFS Status Stratified by Baseline AFS Status (US, ITT) Baseline AFS Status Intergel* Control* n=102 n=98 Minimal/Mild 12/97 11/91 Moderate or Severe 0/5 3/7 * # patients with moderate or severe AFS status at 2nd look divided by # patients with baseline AFS status specified by subgroup
Analysis of AFS Scores (cont.) • Intent-to-treat analysis shows no difference between treatment groups or subgroups • Sponsor’s analysis: Smallest subgroup of patients (< 10% and includes only 5 US Intergel patients) with moderate and severe adhesions drive their evaluable analysis of combined US and European patients
SUMMARY • Sponsor designed an ITT study to evaluate 180 to 200 patients • Sample size met with 200 US patients • US and European data not combinable • ITT analysis of US patients shows no difference between Intergel and Control for mAFS score, # of adhesions, reformed and surgical site adhesions, and AFS status.