Download
1 / 85
870 likes | 1.12k Views
Incontinence and Prolapse. Dr. Jane Schulz Associate Professor Department of Obstetrics and Gynecology University of Alberta. Objectives . At the end of this lecture, you should be able to Describe the prevalence, risk factors and quality of life impact of urinary incontinence

E N D
Incontinence and Prolapse Dr. Jane Schulz Associate Professor Department of Obstetrics and Gynecology University of Alberta
Objectives At the end of this lecture, you should be able to Describe the prevalence, risk factors and quality of life impact of urinary incontinence Explain the two most common types of urinary incontinence Determine the basic treatments for each type of incontinence
Objectives Explain how to diagnose and describe various types of prolapse based on the organ involved Appreciate how urinary incontinence and pelvic organ prolapse are inter-related as defects of the pelvic floor
Definitions Urinary Incontinence Involuntary loss of urine that is a social or hygienic problem
Incontinence The Most Common Cause Of Admission To Long Term Institutionalized Health Care Centres In The United States And Canada
Myths • Urinary incontinence is a natural part of aging • Nothing can be done about it • Surgery is the only solution
Epidemiology • Canadian Continence Foundation data indicates that 1 in 4 women and 1 in 10 men will suffer from urinary incontinence in their lifetime
Prevalence of Urinary Incontinence -- Canada 3.3 million Canadians 7-8% of the population 4X more common in women than men Increases with age General estimates 30% childbearing/premenopausal women 40-50% postmenopausal women 60% nursing home women Canadian Continence Foundation website
Prevalence of female stress incontinence by age Canadian consensus on menopause, SOGC Bulletin, 2006
Prevalence of female urge incontinence by age Canadian Consensus on Menopause, SOGC Bulletin, 2006
Reasons for Underreporting • Less than half of those with bladder control problems report it to their health care provider WHY? • Embarrassment • Low expectations of benefit • Lack of information regarding management options and their success rates • Availability of absorbent products • Physicians do not ask about the problem
OAB: Quality of life (QoL) impact potentiallycomparable to other disease states SF-36 Score Healthy OAB Diabetes 90 80 70 60 50 40 0 Physicalfunction Rolefunction Bodilypain Generalhealth Vitality Socialfunction Emotionalfunction Mentalhealth Abrams P, et al. Am J Manag Care 2000;6(Suppl. 11):S580–90
Association Between Overactive Bladder and Falls/Fractures • Database study of 6049 women over 4 years • daily urge incontinence was independently associated with an increased risk of falls and fractures of 35% and 43% compared with controls • these associations were independent of other measures of functional status Brown JS et al. J Am Geriatr Soc. 2000;48:721-725.
Causes of incontinence Inherited or genetic factors • Race (more common in white women) • anatomic differences • connective tissue (markans syndrome) • neurologic abnormalities (spinibifida)
Causes of incontinence External factors • pregnancy and childbirth • aging • hormone effects • nonobstetric pelvic trauma and radical surgery • increased intra-abdominal pressure • drug effects
Types of urinary incontinence • genuine stress incontinence • urge incontinence • mixed • chronic urinary retention and overflow incontinence • atypical incontinence • miscellaneous (UTI, dementia)
Genuine stress incontinence • loss of urine with increases in abdominal pressure • caused by bladder prolapse or weak sphincter • symptoms include loss of urine with cough, laugh, sneeze, running, lifting, walking
Urge incontinence • loss of urine due to an involuntary bladder spasm (contraction) • complaints of urgency, frequency, inability to reach the toilet in time, up a lot at night to use the toilet • multiple triggers (cough, water, key in door) • 85% idiopathic
Overactive bladder symptoms frequency nocturia urge incontinence urgency Overactivebladder
Mixed incontinence • combination of stress and urge incontinence • common presentation of mixed symptoms • bladder test can help diagnose
Chronic urinary retention/overflow incontinence/voiding dysfunction • outlet obstruction or bladder underactivity • may be related to previous surgery, aging, development of bad bladder habits, or neurologic disorders • can be due to medication, such as antidepressants • may present with symptoms of stress or urge incontinence, continuous leakage, or urinary tract infection
Functional and transient incontinence • especially in the elderly • urinary tract infection • restricted mobility • severe constipation • medication - diuretics, antipsychotics • psychological causes
Causes of Transient Incontinencein the Elderly D elirium, acute confusion I nfection: symptomatic urinary tract infection A trophic urethritis or vaginitis P harmaceuticals P sychological problems E xcessive urine output R estricted mobility S tool impaction Resnick. JAMA. 1996;276:1832-1840.
Unusual causes of urinary incontinence • urethral diverticulum • genitourinary fistula • congenital abnormalities (bladder extrophy, ectopic ureter) • detrusor hyperreflexia with impaired contractility • giggle incontinence • enuresis (bedwetting) • urethral instability
Screening 1. Stress incontinence“Do you have urine leakage at any time?”“Do you ever leak urine when laughing, coughing, sneezing, or with physical exertion?” 2. Urgency“Do you often have to rush to the bathroom or feel like you have to go right away?”“Do you ever leak urine before reaching the bathroom?”
Screening 3. Number of voids“How many trips to the bathroom would you usually have in a 24-hour period?”“Of these, how many are during the day or evening? After bedtime?” 4. Solution?“Is your bladder control a problem for you?”“How bothered are you by this problem?”“There are solutions we can use for bladder control problems, would you like to discuss them?”
Further history Ask about medical conditions/medications that could affect bladder function Diabetes, MS, neurological disease Diuretics, psychiatric drugs O/G Hx Attention to symptoms of atrophy, coital incontinence Social Hx FLUID, FLUID, FLUID smoking
Physical Examination • Physical examination—cough stress test • Clinician observes urethra, while patient in lithotomy position coughs vigorously • Instantaneous leakage—stress incontinence likely • Delayed or persistent leakage—detrusor instability likely • No leakage—repeat test with patient in upright position • Evaluate the integrity of the pelvic musculature Clinical Practice Guidelines: Urinary Incontinence in Adults. 1996. AHCPR publication 96-0682.
The physical exam may include a general evaluation of neurologic status and examination of the abdomen, rectum, genitals, and pelvis. The cough stress test, in which the patient is asked to cough vigorously while the examiner observes the urethra, allows direct observation of any urine loss. When instantaneous leakage results from coughing, stress incontinence is a likely diagnosis. In cases where leakage is delayed or persists after the cough, detrusor instability may be the cause. The cough stress test should be performed initially in the lithotomy position; if no leakage is observed, the test should be repeated with the patient in the upright position.1 • In patients with a positive history, the initial evaluation also includes assessment of the degree of pelvic muscle dysfunction. This is accomplished by review of a patient voiding diary and by palpation of the levator muscle during voluntary contraction on physical examination. Careful pelvic and rectal examinations, an assessment of pelvic floor muscle function, and an assessment of the integrity of the sacral nerves are included in the physical exam.
Urinary Incontinence Treatment • Behavioral • Pelvic muscle rehabilitation • Biofeedback • Electrical stimulation • Bladder training • Pharmacological • Surgical Fantl JA. Urology. 1998;51(suppl 2A):30-34.Abrams, P, Wein AJ. The Overactive Bladder; A Widespread and Treatable Condition. 1998.
There are a number of causes of urge urinary incontinence and a variety of strategies currently employed in its treatment. Behavioral techniques, such as pelvic floor muscle rehabilitation and bladder training, have been demonstrated effective in reducing incontinence,1 as have the use of electrical stimulation2 and surgery.3 Two major categories of behavioral modification are employed in the treatment of urge urinary incontinence1: Pelvic muscle rehabilitation involves implementation of a comprehensive group of progressive exercises aimed at strengthening the levator muscle. These exercises have been used to treat several types of urinary incontinence, but are most frequently employed in patients diagnosed with stress incontinence. The use of biofeedback during exercise allows patients to observe the duration and strength of contractions. Electrical stimulation (nonimplantable) is administered with the help of vaginal or anal sensors or surface electrodes. The stimulation produces a contraction of several muscles (levator ani, external urethral and anal sphincters), accompanied by reflex inhibition of the detrusor muscles.4 Bladder training is a form of behavioral therapy. The aim is to help the patient gain bladder control by increasing the effective capacity of the bladder. Keeping a record of frequency and volume of micturitions is the key, as well as the documentation of the fluid intake. The patient is asked to increase the intervals between voids, which will result in a gradual increase in bladder capacity.2
Prompted voiding • May be helpful in long-term care • Labor intensive • Must be maintained • Effective in 40% cases • Need more research on most cost-effective methods to treat OAB in long-term care setting
Estrogens • Small amount of data on increased MUCP (maximal urethral closure pressure) with local estrogen • Data showing relief of irritative bladder symptoms with local estrogen • Relief of vaginal dryness • Increased success of pessary fitting with local estrogen
Potential of combination therapyPercent reduction incontinence episodes after 8 weeks Burgio et al JAGS 2000
make sure toilet seat height O.K. • If use elevated toilet seat ensure feet still touch the floor • Behavioral Rx still important in elderly • Elevate legs in day/afternoon • Restrict pm fluids • Use diuretics early in the day • Evaluate clothing, corsets/girdles may be interfering with ability to void in time • In elderly have realistic expectations, may aim for q2hrly voids rather than q3-4hrly
Anticholinergic agents Side effects • dry mouth • blurred vision • tachycardia • drowsiness • cognitive impairment • impaired gut motility • contraindicated in patients with narrow angle glaucoma and voiding dysfunction
-wise to check PVR 1-2 weeks after starting anti-cholinergic in elderly • if they get worse may be developing retention • Stop med and then could restart at lower dose • Enough fluids and possibly increased fibre or bowel regime in elderly on anti-cholinergic to avoid causing or exacerbating constipation
Pharmacologic treatment Anticholinergics • Oxybutynin IR (Ditropan) 2.5 to 5mg bid totid • Tolteridine IR (Detrol) 1 to 2mg bid • Oxybutynin ER (Ditropan XL) 5 to 15mg qd • Tolteridine ER (Detrol LA) 2 to 4mg qd • Oxybutynin patch (Oxytrol) 1 patch twice per week • Solifenacin (Vesicare) 5 or 10 mg qd • Darifenacin (Enablex) 7.5 or 15mg qd • Trospium (Trosec) 20mg bid • Oxybutynin CR (Uromax) 10 to 15mg qd
Botulinum toxin for IDO • Multiple studies demonstrating efficacy of BoNT for refractory IDO and NDO • 5-9 month effect • Dose related retention • Technique not yet standardized
Stress Fluid management Physiotherapy Pessary Local HRT Urethral plug Bulking agents TVT/TOT/Burch/sling Urge Bladder retraining Urge suppression Fluid management Physiotherapy Anticholinergic medication Local HRT Botox Urinary Incontinence Treatment
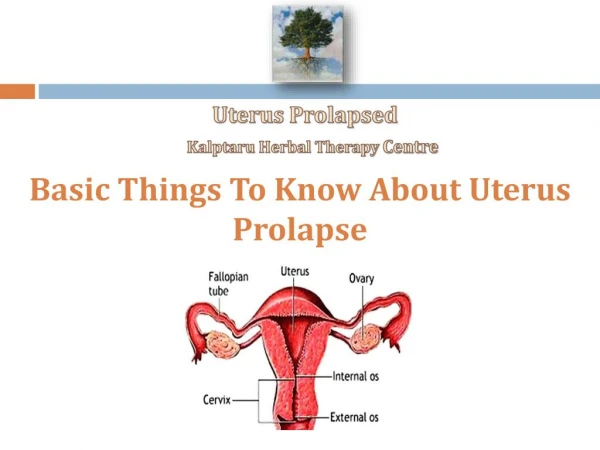
Pelvic organ prolapse • pelvic organs protruding through the vagina • each component named according to protruding organ
Prevalence 50% of parous women have some degree of prolapse 2-3% of women seek help for prolapse 1/2 of women with severe POP never present to physicians
Risk Factors Parity/vaginal delivery advanced age (post-menopausal) Obesity Chronic coughing/straining Hysterectomy Bladder surgery
Types of prolapse • cystocele (bladder) • rectocele (rectum) • enterocele (cul-de-sac peritoneum or small bowel) • uterine prolapse • vaginal vault prolapse