Download
1 / 43
430 likes | 444 Views
Learn about Adaptive Servo-Ventilation (ASV) technology, its effectiveness in treating central sleep apnea, and the latest advancements in BiPAP therapy. Understand the key features, indications, and mask options for ASV devices. Stay informed on Medicare coverage guidelines for sleep apnea treatments.

E N D
Adaptive servo-ventilation (Anticyclic Modulated Ventilation) BYAHMAD YOUNESPROFESSOR OF THORACIC MEDICINE Mansoura Faculty of Medicine
Adaptive Servo Ventilation • Adaptive servo-ventilatio (ASV) is a form of "BiPAP". The difference is that ASV varies IPAP and/or EPAP to adjust ventilation as needed by the patient. • With traditional BiPAP the pressures are set and don't vary. • At some point in the late 1990sResMed Corporation developed an ASV machine, and had it tested in heart failure patients with Cheyne-Stokes respiration. C-S respiration, often occurs during sleep in patients with congestive heart failure. • The first clinical article to appear on ASV wasTeschler H, et al. Adaptive pressure support servo-ventilation: a novel treatment for Cheyne-Stokes respiration in heart failure. 2001. • Over the next decade more articles appeared showing that ASV could treat not only Cheyne-Stokes respiration, but a syndrome that wasn't even recognized in 2001: Complex Sleep Apnea. Principal Indications 1) Central sleep apnea unresponsive to CPAP or BiPAP. 2) Complex sleep apnea.
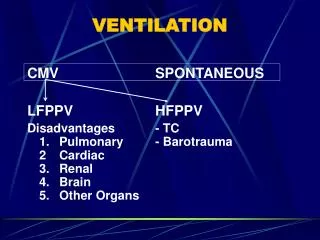
BiPAP sets two pressures above the ambient, a higher (IPAP) and a lower (EPAP), e.g., 10/5 cm H2O. In BiPAP the higher pressure is experienced on inspiration and the lower pressure on expiration. Note that both pressures are always above ambient.BiPAP is equivalent to PSV (pressure support ventilation) + PEEP (positive end-expiratory pressure) in the intubated patient; in that situation PEEP is the same as EPAP.
Autobilevel positive airway pressure with a minimum (EPAP) of 6 cm H2O and a maximum (IPAP) of 25 cm H2O.
ASV is a variant of BPAP that was developed to treat Cheyne-Stokes central apnea. Both ASV and BPAP devices with a backup rate are approved for use with patients with central apnea and complex sleep apnea
The ASV device responds to variation in flow by increasing PS when flow and ventilation are low and decreasing PS when flow is high.
Servoventilation devices Three servoventilation devices are in current clinical use :VPAP-AdaptSV (ResMed Corp, San Diego, CA) ,BiPAP-AutoSV (Respironics, Murraysville, PA) and SomnoVent CR Algorithms of action for either VPAP-AdaptSV ,BIPAP AutoSV or SomnoVent CRare proprietary and not accessible to the medical community.
What kind of mask is used? • ResMed specifies their brand of full face mask for the ResMed VPAP Adapt SV machine. • ResMed VPAP Adapt SV: EPAP [expiratory positive airway pressure] = 7.0 cm H2O, Minimum PS [pressure support] = 4.0 cm H2O, Maximum PS = 13.0 cm H2O, via ResMed Quattro Full Face Mask (mask recommended by ResMed with this machine), with heated humidity. • Respironics autoSV: EPAP [expiratory positive airway pressure] = 7.0 cm H2O, Minimum PS [pressure support] = 4.0 cm H2O, Maximum PS = 13.0 cm H2O. Respironics states their machine can be used with virtually any mask. • Note: Respironics has an upgraded version of auto SV, called autoSV Advanced. The auto SV Advanced machine allows the EPAP to vary along with the PS (pressure support) level. In the auto SV you would set a lower and higher EPAP, e.g., EPAP-min = 7, EPAP-max = 12.
Medicare Coverage Guidelines • for Central sleep apnea, defined as: 1. Study showing AHI > 5 events/hr. and 2. Central apneas/hypopneas greater than > 50% of the total apneas/hypopneas, and 3. Central apneas or hypopneas >=5/hr., and 4. Symptoms of either excessive sleepiness or disrupted sleep. • for Complex sleep apneaCompSA is a form of central sleep apnea specifically identified by the persistence or emergence of central apneas or hypopneas upon exposure to CPAPor Bi-level device when obstructive events have disappeared. These patients have predominantly obstructive or mixed apenas during the diagnostic sleep study occurring at >= 5 times per hour. With use of a CPAP or Bi-level, they show a pattern of apneas and hypopneas that meets the definition of CSA described above.
ASV is a CONFUSING term, for several reasons. 1)It is a manufacturers' proprietary trade mark,owned by ResMed Corporation. ResMed was the first company to come out with this type of 'smart' machine, which is designed for treatment of central sleep apnea and complex sleep apnea. 2) Another equipment company, Philips Respironics, has come out with a competing machine for the same set of conditions. Respironics calls its machine BiPAP-autoSV, which stands for 'automatic servo ventilation.' Obviously this is also 'ASV' butRespironics can't market their machine as 'ASV' and they always use the term "autoSV". 3)The algorithms that govern these machines are both proprietary, which means they can't be duplicated by any other machines on the market. 4)The manufacturers use a variety of abbreviations, often without explanation, in their brochures and web sites. Sometimes they use "EEP" (end-expiratory pressure) to indicate what is more commonly called "EPAP" (expiratory positive airway pressure), and "PS" (pressure support) to indicate "IPAP" (inspiratory positive airway pressure). In summary, ASV-type machines are an evolving technology, and the terminology is not as well defined as it is with BiPAP and CPAP.
Adaptive servo-ventilation • Central sleep apnea (CSA) and periodic breathing is frequently—but not only—found in patients with chronic heart failure (Cheyne-Stokes respiration,CSR) due to ischemic heart diseases, dilated cardiomyopathy or arterial hypertension. • Different studies showed a proportion of up to 50% of heart failure patients affected with sleep-disordered breathing. However, many of these patients do not only present with central disturbances or periodic breathing but also suffer from obstructions of the upper airways . • CPAP is the treatment of choice for obstructions of the upper airways during sleep.CPAP attenuates central breathing disturbances during sleep and improves heart function and quality of life in heart failure patients with OSAS .CPAP has been shown to reduce the figures of central disturbances by 50%. • ASV has been developed to more effectively improve CSA/CSR.
Adaptive servo-ventilation • The algorithms of ASV increase the pressure during hypopneas and reduce it during hyperventilation. • ASV has been shown to improve respiratory disturbances in patients with CSA/CSR, complex sleep apnea and mixed sleep apnea, and to be significantly more effective than CPAP, bi-level therapy, non-invasive ventilation, and oxygen • For patients with OSA, auto-adjusting CPAP (APAP) devices were developed with the aim of achieving optimal adaptation of the treatment pressure to the actual requirement of the patients. • APAP reduces the treatment pressure substantially and is preferred by patients. • combination of adaptive servo-ventilation and automatically adjusting CPAP might be the optimal treatment for patients with both Cheyne-Stokes respiration and OSAS.
What are the principal uses in the ACUTE SETTING? ASV via face mask is not used in the acute setting. ASV as a ventilatory mode in intubated patients is used occasionally. One study (Intensive Care Med. 2010 Aug;36(8):1371-9. Epub 2010 May 26. Adaptive support ventilation versus conventional ventilation for total ventilatory support in acute respiratory failure. Iotti GA, et. al.) found that "Comparison between ASV and CV [controlled ventilation] resulted either in similarities or in minor differences. Except for excessive Vt in a few obstructed patients, all differences were in favor of ASV.“ ASV is currently used almost exclusively in the NON-ACUTE SETTING setting, for patients with'complex sleep apnea'. CompSA, Thus, ASV is indicated for situations when CPAP or BiPAP has failed. Even so, it remains somewhat unsettled about when ASV should be used, how effective it is, and how to follow up such patients.
Principal Indications • There are two principal indications: 1)Central sleep apnea 2) Complex sleep apnea. • Central sleep apnea can basically be divided into Cheyne-Stokes (C-S) and non-Cheyne Stokes breathing.
What kind of mask is used to deliver ASV? ResMed recommends their full face mask. Shown below is the ResMed Quattro Pro full face mask.
ResMed VPAP Adapt SV: Backup rate: 12 breaths/minute Rise time: (the time it takes the device to change from EPAP to IPAP. Settings range from 1 [fastest] to 6 [slowest]. The range of values corresponds to 1/10 seconds, so that a rise time of 4 = 0.4 seconds) Inspiratory time: 2 seconds (range is 0.5 to 3.0 seconds) EPAP [expiratory positive airway pressure] = 7.0 cm H2O Minimum PS [pressure support] = 4.0 cm H2O Maximum PS = 13.0 cm H2O Maximum pressure for device (generally <=30 cm H2O) Mask: ResMed Quattro Full Face Mask (recommended by company for their ASV machine), with heated humidity
Costs ResMed's VPAP Adapt SV is probably the same price as Respironics AutoSV machine, which is $5800. In addition there is the cost of the mask, and also the sleep studies needed before any machine can be prescribed.
Respironics AutoSV ASV" as a label and a particular methodology to adjust pressures was patented by ResMed. A few years later, another large equipment manufacturer, Philips Respironics, came out with their own ASV-type machine; they call it "autoSV." Auto SV is also an adaptive servo ventilator device that uses a different algorithm to adjust bilevel pressures. A newer model is called Auto-SV Advanced.
The device tracks flow. "The flow signal is analyzed and a target flow is calculated. If the patient reaches the flow target, the device does not offer any additional pressure support. If the patient does not reach the flow target the device will dynamically change pressure support breath to breath .The device tracks peak flow over a 4-minute cycle, as shown below.
A peak flow target is established around the 4-minute average and the machine changes the air delivery as needed, to deliver 90% of the target, as shown below.
Below is the pressure curve from Repironics regular AutoSV machine, taken from a Respironics bronchure .
Principal Indications 1-Central sleep apnea 2-Complex sleep apnea What kind of mask is used to deliver ASV? • Respironics states any mask used for CPAP should work with their auto SV machine. • Below is the Respironics Comfort Gel full face mask.
Respironics AutoSV Respironics currently has TWO devices, the regular AutoSV and the AutoSV Advanced. Respironics recommends that physcians now prescribe ONLY the AutoSV Advanced, so it seems likely that the regular machine will be phased out soon. Regular Auto SVFor the regular AutoSv you can use the same prescription example as listed under ResMed.
SOMNOvent CR • Respiratory disturbances are detected based on the analysis of actual minute ventilation, flow profile and snoring. • The minute ventilation is compared with the average minute ventilation in a moving window • The treatment mode is called anticyclic modulated ventilation (ACMV).
The difference between IPAP and EPAP defines the tidal volume. The EEPAP varies automatically due to the level of the upper airway obstruction
Variation of treatment pressures during Cheyne-Stokes respiration. During hypopneas the difference between IPAP and EPAP progressively increases, while there is no inspiratory pressure support during hyperventilation. When the patient breathes normally the pressure is relieved in expiration. The user has to set the lower level of the EEPAP and the upper limit of the IPAP.
SOMNOvent CR • Device which combines automatic CPAP and adaptive servo-ventilation proved to effectively suppress all types of upper airway obstructions, such as snoring, obstructive apneas and hypopneas. Moreover, central respiratory disturbances including periodic breathing were deleted , and sleep quality improved. • The results did not differ whether or not patients suffered from cardiovascular diseases.
The device incorporates different features for treating breathing disturbances non-invasively. • It automatically adapts the positive airway pressure at the end of the expiration, as this period of the breathing cycle is critical for the opening of the upper airways.This component represents the automatic CPAP mode which has proven effective in the treatment of OSAS. • In periods of normal breathing the expiratory pressure is relieved. • The device applies varying tidal volumes which are defined by the difference between IPAP and EPAP (pressure level in the early expiration period). Thus, periodic breathing is overcome by increasing the tidal volume during central hypopneas and decreasing it during hyperventilation. • Mandatory breaths are applied if there is complete cessation of the airflow due to central apneas. • The back-up frequency has been designed to avoid inducing hypoventilation.
While apneas can be identified undoubtfully in most cases, central and obstructive hypopneas might be difficult to discriminate based on standard polysomnographic parameters. • Esophageal pressure is hardly accepted in clinical settings and re-evaluation studies. • Therefore, we scored central hypopneas based on the analysis of the inspiratory flow curve and the pattern of the effort parameters., • One important advantage of the here presented algorithm is the automatic discrimination between obstructive and central disturbances and the consecutive automatic adaptation of the end-expiratory pressure. • Many patients with OSAS present with at least a minor portion of central disturbances, and CPAP or bi-level therapy may induce CSA/CSR.
The co-existence of obstructive and central disturbances likely represents the common pathophysiology . Thus, central apneas have been found to be frequently accompanied by upper airway occlusion ; periodic breathing in hypoxic conditions results in upper airway narrowing . • In heart failure, there is evidence for an overnight shift in predominance of obstructive apneas to central apneas . • Similar to upper airway obstructions, central apneas increase in the supine position and can be reduced under CPAP treatment. For these aspects a trial of CPAP can be recommended as first step in the treatment of patients with co-existing obstructive and central disturbances.
Complex sleep apnea syndrome Several studies have shown that central apnea activity may disappear with continued CPAP use in a subset of patients. Based on that, it has been postulated that in a subset of patients, ‘‘complex sleep apnea’’ may then merely reflect difficulty adjusting to the PAP with repeated ‘‘transitional’’, sleep-onset central apneas, inadequate titration or over titration of PAP, or substantial mask leak. There are a number of patients with complex apnea patients who continue to have central apnea activity even after years of CPAP use
If complex sleep apnea ("Comp SA") is a result of CPAP, BiPAP may be tried, though it is not usually successful. When Comp SA doesn't respond to BiPAP, or is a result of BiPAP in the first place, there are two choices: a) Continue CPAP or BiPAP to treat the OSA, hoping that the central apneas will remit over time (they sometimes do); b) Start the patient on ASV. There is no clear standard about when to start ASV on patients who manifest Comp SA. Mask type and size is best determined in the sleep lab, when a patient is being titrated on an ASV machine.
Conclusions ASV is a way station on the road to newer and smarter machines. Expense (about $6000 per machine) limits their wider use, but no doubt these machines will become cheaper and at some point replace our basic CPAP/BiPAP units. Despite the fact that the proprietary algorithms are rather opaque, three machines seem to work well in their stated objectives of treating central sleep apnea and complex sleep apnea. As such, they compete in the market for treatment of these conditions. From the standpoint of the sleep medicine specialist, neither machine is clearly superior or inferior.
Conclusions Since ResMed was first out with an ASV machine, most of the articles in the medical literature are based on ResMed's device, but there are now several publications for autoSV and Somnovent CR as well. More importantly, this is a rapidly evolving field, and new machines will likely appear soon, from these three companies as well as other competitors.