Download
1 / 21
210 likes | 348 Views
Psychopharmacological interventions for ADHD. Dr. Charles Pemberton, Ed.D, LPCC Manbeena Sekhon, Doctoral Student. Today’s plan. Not a complete presentation. Talk to your MD Why Study? ADHD Basic Elements of: Methylphenidate Dextroamphetamine Atomoxetene When to use which.

E N D
Psychopharmacological interventions for ADHD Dr. Charles Pemberton, Ed.D, LPCC Manbeena Sekhon, Doctoral Student
Today’s plan • Not a complete presentation. Talk to your MD • Why Study? • ADHD • Basic Elements of: • Methylphenidate • Dextroamphetamine • Atomoxetene • When to use which.
Why Should Non-prescribers know this? • Education • Weekly monitoring • Side-effect intervention • Diagnosing • Timing • Reputation, future referrals
Attention Deficit Hyperactivity Disorder • Within the “Disorders Usually First Diagnosed in Infancy, Childhood, or Adolescence” grouping, then subgrouped by the category of “disruptive or self injurious behavior”
ADHD, Major Diagnostic Features • Often will not complete tasks • Easily distracted by minor stimuli • Work often messy and completed w/o thought • Forgetful in day-to-day activities • Impulsive (interrupting others, cannot wait turn, etc.) • Fidgetiness • Excessive talking
Prevalence of ADHD • Estimated at 3-7% of school age children • More common in males than females • Often diagnosed during elementary school years.
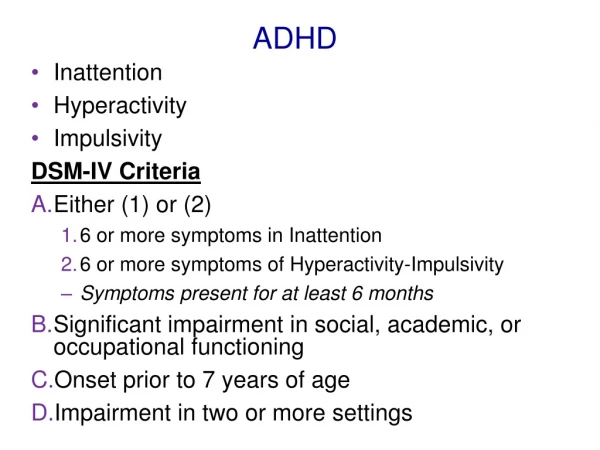
Subtypes of ADHD • 314.01 ADHD, Combined Type • Criteria A1 & A2 both met for past 6 months • 314.00 ADHD, Inattentive Type • Criteria A1 met, but not A2 • 314.01 ADHD, Hyperactive-Impulsive Type • Criteria A2 met, but not A1 • 314.9 ADHD NOS • Prominent symptoms but do not meet diagnostic criteria
Diagnostic Criteria for ADHD • A 1. Must exhibit 6 or more symptoms of inattention, persisting for minimum of 6 months: from list of 9 items, a through i. • fails to give close attention to details • often has difficulty sustaining attention • often does not seem to listen when spoken to directly • often has difficulty organizing tasks and activities • often loses things necessary for tasks • often easily distracted by extraneous stimuli • often forgetful in daily activities
Diagnostic Criteria, cont’d: • A 2. Must exhibit 6 or more symptoms of hyperactivity-impulsivity, persisting for minimum of 6 months, from list of 9 items, a through i. • often fidgets with hands or feet or squirms in seat • often leaves seat in classroom • often runs about or climbs excessively • is often "on the go" or often acts as if "driven by a motor“ • often talks excessively • often blurts out answers • often has difficulty awaiting turn • often interrupts or intrudes on others
Diagnostic Criteria, cont’d: • B. symptom onset PRIOR to age 7 years • C. impairment present in two or more environments • D. clear clinically significant impairment in functioning • E. cannot be accounted for by other mental disorder
Basic Elements of Methylphenidate • Known as: Ritalin, Ritalin SR, Ritalin LA, Concerta, Metadate ER, Metadate CD, Focalin • Pharmacology: It is a CNS stimulant, which is chemically related to amphetamine • Preparations – 5, 10, 20 mg tabs; sustained release 20 mg tabs; LA 20, 30, and 40 mg capsules. The SR tablet should be swallowed and not crushed or chewed. Concerta comes in 18 and 36 mg extended release tablets. Metadate CD 20 mg capsules; Metadate ER 10 – and 20 – mg tabs. Focalin 2.5, - 5-, 10 - mg tabs.
Methylphenidate, cont’d • Half-Life – 3-4 hours; 6-8 hours for sustained release • It’s a schedule II controlled substance, requiring a triplicate prescription • Pre-Drug Work-Up • Blood pressure and general cardiac status • baseline and periodic blood counts and liver function tests • Weight and growth should be monitored in children
Methylphenidate, cont’d • Adverse Drug Reactions • Nervousness and insomnia; can be reduced by decreasing dose. • Cardiovascular – Hypertension, tachycardia, and arrhythmias. • CNS – Dizziness, euphoria, tremor, headache, precipitation of tics and Tourette’s syndrome, and rarely psychosis. • GI – Decreased appetite, weight loss. • Case reports of elevated liver enzymes and liver failure. • Hematological –Leukopenia and anemia have been reported • Growth Inhibition
Basic Elements of Dextroamphetamine • Known as: Adderall, Adderall XR • Pharmacology:causes the release of norepinepherine from neurons. At higher doses, it will also cause dopamine and serotonin release • Preparations – Adderall 5-, 7.5-, 10-, 12.5-, 15-, 20-, 30-mg tablets; Adderall XR 5-, 10-, 15-, 20-, 25-, 30-mg capsules.
Dextroamphetamine, cont’d • Half-Life – 10-25 hours • It’s a schedule II controlled substance, requiring a triplicate prescription • Pre-Drug Work-Up • Blood pressure and general cardiac status should be evaluated prior to initiating dextroamphetamine. • Can precipitate tics • Contraindicated in in patients with hypertension, hyperthyroidism, cardiac disease or glaucoma. It is not recommended for psychotic patients ot patients with a history of substance abuse. • Weight and growth should be monitored in all children.
Dextroamphetamine, cont’d • Adverse Drug Reactions • Side effects – most common side effects are psychomotor agitation, insomnia, loss of appetite, and dry mouth. Tolerance to loss of appetite tends to develop. Effect on sleep can be reduced by making sure no drug is given after 12 pm. • Cardiovascular – Palpitations, tachycardia, increased blood pressure. • CNS – Dizziness, euphoria, tremor, precipitation of tics, Tourette’s syndrome, and rarely, psychosis. • GI – Anorexia and weight loss, diarrhea, constipation. • Growth inhibition
Basic Elements of Atomoxetene • Known as: Strattera • Pharmacology:works via presynaptic norepinepherine transporter inhibition • Preparations – 10, 18, 25, 40, and 60 mg capsules .
Atomoxetene, cont’d • Half-Life – approximately 4 hours • Not a schedule II controlled substance • Clinical Guidelines – • Dividing the dose may reduce some side effects • Dose reductions are necessary in presence of moderate hepatic insufficiency • Atomoxetine should not be used within 2 weeks of discontinuation of a MAO inhibitor. • Atomoxetine should be avoided inpatients with narrow angle glaucoma and, it should be used with caution in patients with tachycardia, hypertension, or cardiovascular disease. • It can be discontinued without taper. • Pregnancy C category.
Atomoxetene, cont’d • Adverse Drug Reactions • Cardiovascular – increased blood pressure and heart rate (similar to those seen with conventional psychostimulant). • BI – Anorexia, weight loss, nausea, abdominal pain. • Miscellaneous – Fatigue, dry mouth, constipation, urinary hesitancy and erectile dysfunction.
When to use, when to change • Side effects • Past history • Substance abuse • Efficacy • Onset time • Stimulant first line, Strattera second • Follow MD
Closing Thoughts • Stimulants still first line defense • Look at choice of drug based upon time of release • Be aware of study sponsor • Addictive nature • Subscribe to Medscape