Download
1 / 25
300 likes | 743 Views
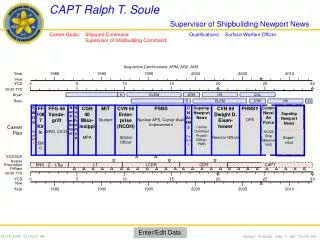
Ralph T. Soule, Captain, US Navy, retired Division Director Aircraft Carrier Test, Evaluation, and Certification Naval Sea Systems Command ralph.soule@gmail.com www.ralphsoule.com. Lessons from the Loss of THRESHER. High Reliability for Patient Safety.

E N D
Ralph T. Soule, Captain, US Navy, retired Division Director Aircraft Carrier Test, Evaluation, and Certification Naval Sea Systems Command ralph.soule@gmail.com www.ralphsoule.com Lessons from the Loss of THRESHER High Reliability for Patient Safety DISTRIBUTION STATEMENT A: Approved for public release; distribution is unlimited.
Submarine Maintenance and Medical CareSimilar Attributes • Highly regulated • Safety is essential – severe consequences for failure • Operating environments are inherently hazardous • Complex, interdependent systems • People play a critical role in complex processes • Highly reliable, long-term operations are essential • Learning from experience is essential
Submarine Maintenance and Medical CareSimilar Attributes • Most of our “patients” don’t really want to see us • Our families have no idea what we’re talking about when we discuss work • We use a lot of hoses, gases, and electrical connections in our work • When something gets in our way, we just make an “incision” to move it • Workers wear strange clothing
Submarine Maintenance and Medical CareDifferences • Ship’s cannot “elope” from shipyards • Shipyard maintenance involves teams of hundreds, up to thousands of people • Shipyard managers and engineers never say “this won’t hurt a bit” • The “patient” is awake the whole time and often gives us instructions to help us do the job “better”
Submarine Safety Culture A Requirement An Attitude A Responsibility
Outline History - Loss of THRESHER High Reliability Lessons: Submarine Safety (SUBSAFE) and other maintenance processes Applications to Medical Care
Early Submarine LossesSubmarines Lost 1915-1963 17 submarines lost to non-combat causes 1915: USS F-4 (SS-23) 1917: USS F-1 (SS-20) 1920: USS H-1 (SS-28) USS S-5 (SS-110) 1923: USS O-5 (SS-66) 1926: USS S-51 (SS-162) 1927: USS S-4 (SS-109) 1939: USS SQUALUS (SS-192) 1941: USS O-9 (SS-70) 1942: USS S-26 (SS-131) USS R-19 (SS-96) 1943: USS R-12 (SS-89) 1944: USS S-28 (SS-133) 1949: USS COCHINO (SS-345) 1958: USS STICKLEBACK (SS-415) 1963: USS THRESHER (SSN-593) 1968:USS SCORPION (SSN-589) 470 Lives Lost
USS THRESHER (SSN-593) • Laid down, 28 May 1958, at Portsmouth Naval Shipyard, Kittery, ME. • Launched on 9 July 1960. • 13th nuclear powered attack submarine. • The first ship of its Class; leading edge of US submarine technology: • combining nuclear power with modern hull design • newly-designed equipment and components USS THRESHER launching ceremonies at the Portsmouth Naval Shipyard, Kittery, Maine, 9 July 1960. She was fast, quiet, and deep diving
On April 10, 1963, while engaged in a deep test dive, approximately 200 miles off the northeastern coast of the United States, the U.S.S. THRESHER (SSN-593), was lost at sea with all persons aboard - 112 naval personnel and 17 civilians. PNSY THRESHER wreckage: About 200 miles off Cape Cod in 8,400 ft of water
Navy Response to Loss of USS THRESHER • Immediately limited diving depth of all submarines • Court of Inquiry • THRESHER Design Appraisal Board • Focus: • Design • Construction • Operation • Testimony Before Congress
Investigation Conclusions Flooding in the engine room Unable to securefrom flooding Spray on electrical switchboards Unable to blow ballast tanks Loss of propulsion power
Inception of the SUBSAFE and Significant Culture Change LOSS of THRESHER Overhaul/Construction SUBSAFE PROGRAM MAINTENANCE PROCESS CHANGES
Key Lessons “The loss of the Thresher should not be viewed solely as the result of failure of a specific braze, weld, system, or component, but rather should be considered a consequence of the philosophy of design, construction, and inspection … it is important that we reevaluate our present practices where, in the desire to make advancements, we may have forsaken the fundamentals of good engineering. ” – ADM Rickover
Key Lessons • Safety must be part of process design, not an afterthought • Key systems were under-designed for knowable risks • Failure to bound an unexpected problem • An attitude that specifications were merely goals, did not need to be taken literally, and HQ permission not needed for failure to meet them • Impact of accumulated conditions, not a single failure • The Navy had not updated its way of doing business to meet the requirements of updated technology and high-performance ships that could operate in riskier environments • Processes are only as good as their audit plan
Navy High Reliability Practices Applied to Health Care • It is expensive and costly to wait for mistakes to learn • Use existing debriefing records to tune awareness • Safety is created in the moment, where work is done, by the people doing it • “High reliability is a continuous, ongoing, dynamic accomplishment." • The blindness of hindsight bias short circuits learning ...
Navy Maintenance Tools for Medical Care • Checklists • Work Model: training, procedures, supervision • Critiques/Fact Sheets • Risk Management • Audits/Surveillances • Pre-operative safety briefings • Post-event/procedure debriefs
Pre-evolution briefs • Key: interactivity among participants • Overview of procedure, team members, risks, constraints, anomalies, expected outcomes • Each person • Name • Role • What they need(from whom) • What they provide(to whom) • Reports to make (exact phraseology is important) • Reports needed • What was learned from last time • Mostly likely problems and responses (what ifs?)
Post-action reviews (informal) • Key: capturing each person’s perspective, follow up • Was the desired outcome achieved? • Things to do more often • Things not to do next time • Hazards caught (which ones remain open?) • Assess work process tools (effectiveness/utility of pre-briefs, procedure, especially things not covered, but should be, training/qualifications -> management credibility rests with follow up) • What were the surprises and how were they identified? • Things to do differently next time
Understanding the Challenge WHERE YOU THINK YOU ARE THE BATTLE Optimum SAFETY LEVEL WHERE YOU REALLY ARE Minimum ACCIDENT - Actual TIME - Perceived
Submarine Safety Culture A Requirement An Attitude A Responsibility
“Those who cannot remember the past are condemned to repeat it.” - George Santayana “A good pre-event briefing beats an accident investigation any day.” - ADM Kinnaird R. McKee