Download
1 / 81
850 likes | 1.28k Views
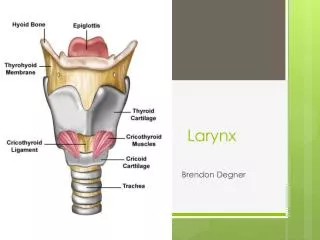
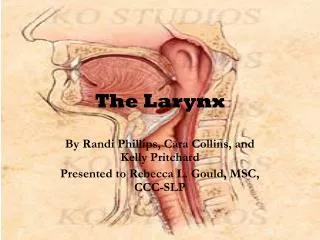
LARYNX. Anatomy . Skeleton Thyroid cartilage Cricoid cartilage Arytenoid cartilage Epiglottis Corniculate cartilage Cuneiform acrtilage. Nerve supply. -from the VAGUS NERVE Superior laryngeal nerve

E N D
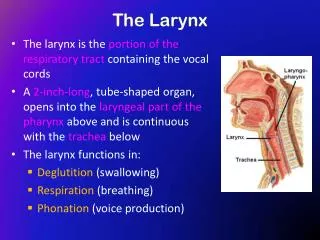
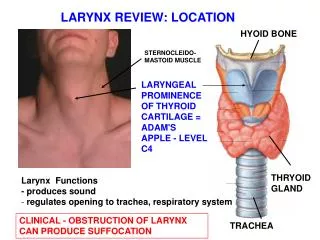
Anatomy Skeleton • Thyroid cartilage • Cricoid cartilage • Arytenoid cartilage • Epiglottis • Corniculate cartilage • Cuneiform acrtilage
Nerve supply -from the VAGUS NERVE • Superior laryngeal nerve motor: extrinsic laryngeal muscle (anterior cricothyroid) and its external branches sensory: mucosa of the upper larynx including glottic plane • Recurrent laryngeal nerve motor: supplies all the intrinsic muscles of the larynx sensory: fibers to the layngeal mucosa below the glottis and to the tracheal mucosa
Blood supply: Arterial • Supraglottic and glottic levels: superior laryngeal artery from ECA • Subglottic: inferior layngeal coming from the subclavian and thyrocervical trunk
Blood supply: venous • Superior thyroid vein drains into IJV • Inferior thyroid vein drain into Branchiocephalic vein
Croup symtoms Croup syndrome: inspriratorystridor caused ny inflammation of the latyngeal or subglotticstenosis. Respiratory distress, cough, and hoarseness True droup: diptheria Pseudocroup: viral, bacterial, spastic forms of the subglottic laryngitis
Vocal Cord Nodules • Usually bilateral • Anterior or middle third of true vocal cord • Any age group • Prevent the vocal folds from meeting in the midline and thus produce hourglass deformity on closure resulting in a raspy breathing voice • Hoarseness or voice changes • Related to chronic voice abuse • Microlaryngeal surgery
Vocal Cord Polyps • Usually single • Middle third of true vocal cord, but may originate from the ventricular area • Locating in the phonating margin of the vocal folds and prevent the vocal folds from meeting in the midline • Male • Sessile, raspberry-like, pedunculated • Related to chronic voice abuse, infection, ETOH, smoking, hypothyroidism • Hoarseness or voice changes
Laryngocele • Abnormal dilatation of the saccule (appendix of the ventricle) containing air and maintaining an open communication with laryngeal lumen • Men >women • Bilateral - 25% • Hoarseness, lateral neck mass, dyspnea, dysphagia, laryngopyocele (pain)
Laryngocele: Types • Internal: laryngocele confined to the intrinsic larynx • External: dilated sac projects upward and laterally • Combined
Laryngocele: Etiology • Acquired: increased intralaryngeal pressure (glassblowers, musicians, weight lifters) • Congenital • SCC in 15% of cases
Laryngocele • Smooth -surfaced, sac-like structure usually filled with air
Laryngocele • Respiratory epithelial-lined (ciliated, columnar) cyst with a fibrous wall • Squamous metaplasia • Oncocytic metaplasia
Contact Ulcers of the Larynx (Pyogenic Granuloma of the Larynx) • Benign, tumor-like condition, occurring most commonly along the posterior aspect of one or both vocal cords • Men>Women, usually adults • Hoarseness, dysphagia, sore throat, dysphonia, difficulty breathing, choking, pain • Etiology: vocal abuse, acid regurgitation, postintubation trauma
Contact Ulcers of the Larynx (Pyogenic Granuloma of the Larynx) • Ulcerated, polypoid, nodular, or fungating mass with a beefy red to tan-white appearance, up to 3 cm in diameter
Laryngeal Amyloidosis • Extracellular, eosinophilic, amorphous material deposited randomly throughout submucosa; depositions around or within the walls • Disappearance of the seromucous glands, • Mixed chronic inflammatory infiltrate
Laryngeal Amyloidosis • Congo red: apple-green birefringence under polarized light
Subglottic Stenosis • Congenital or acquired • Rare; acquired > congenital • Progressive respiratory difficulty, stridor, dyspnea, air hunger, hoarseness, abnormal cry, aphonia, dysphagia • Etiology: trauma, neoplasms, infectious or autoimmune diseases, idiopathic
Subglottic Stenosis • Narrowing of the endolaryngeal diameter with mucosal or submucosal mass or bulging • Histologic picture depends on the cause • Idiopathic stenosis: submucosal fibrous proliferation with associated non-specific chronic inflammation • Differential diagnosis: infectious diseases, Wegener’s granulomatosis, collagen vascular diseases, neoplasms
Laryngeal Papilloma • Benign, exophytic neoplastic growth composed of branching fronds of squamous epithelium with fibrovascular cores • The most common benign laryngeal neoplasm • No sex predilection • Changes in phonation, dyspnea, cough, dysphagia, stridor • HPV types 6 and 11
Laryngeal Papilloma • Juvenile type: multiple lesions with extensive growth and rapid recurrence, may remit spontaneously or persist into old age • Adult type: more often single, recurs less often, less likely to spread
Papillary fronds of multilayered benign squamous epithelium containing fibrovascular cores • Little or no keratin production
Laryngeal Papilloma • Absence of stromal invasion • Certain degree of cellular atypia • Koilocytic changes
Laryngeal Granular Cell Tumor • Men > women • Hoarseness • Along the posterior aspect of true vocal cord ( but also in supraglotic and infraglotic areas)
Granular Cell Tumor • Solitary, polypoid, sessile, papillary, or cystic lesion, measuring up to 3.0 cm in diameter
Granular Cell Tumor • Poorly circumscribed subepithelial lesion with syncytial, trabecular, or nested growth pattern • Round to polygonal cells with round to vesicular nuclei and coarsely granular cytoplasm. Poorly defined cell borders. • Variable degree of cellular pleomorphism • Absence of mitoses or necroses
Granular Cell Tumor • Cytoplasmic granules: PAS/d +, Alcian blue pH 2.5 +, trichrome + (red) • Angulate bodies: needle shaped, PAS + bodies in the interstitial cells • Tumor cells: S-100+, NSE + • Interstitial cells with angulate bodies: S-100 - and myelin protein + • EM: membrane bound autophagic vacuoles containing mitochondria, RER, myelin, axon-like structures
Malignant Granular Cell Tumor • Rare ( 1% of all GCT) • Do not occur in newborns • Size > 4 cm • Increased cellularity, pleomorphism, necrosis, prominent nucleoli, spindle shaped cells and > 2 mitoses/10 HPF • Metastasize via lymphatics and blood vessels
Chordoma • Uncommon • Males > females • Dyspnea, strydor, and hoarseness • May originates from epiglottis, cricoid, arytenoid, or thyroid cartilages • May arise in Reinke’s space • Lobulated, firm to hard, blue-gray, submucosal mass, usually < 1 cm
Chordoma • Lobulated, normally looking chondrocytes • Absence of pleomorphism, binucleated chondrocytes, or mitotic activity
In Situ Squamous Cell Carcinoma • Males > females • 6th – 7th decades • Most often involves anterior portion of true vocal cord • Hoarseness • May coexist with invasive SCC • May be isolated or multifocal • Circumscribed or diffuse lesion with a white, red, or gray color and smooth or granular appearance