Download
1 / 1
100 likes | 517 Views
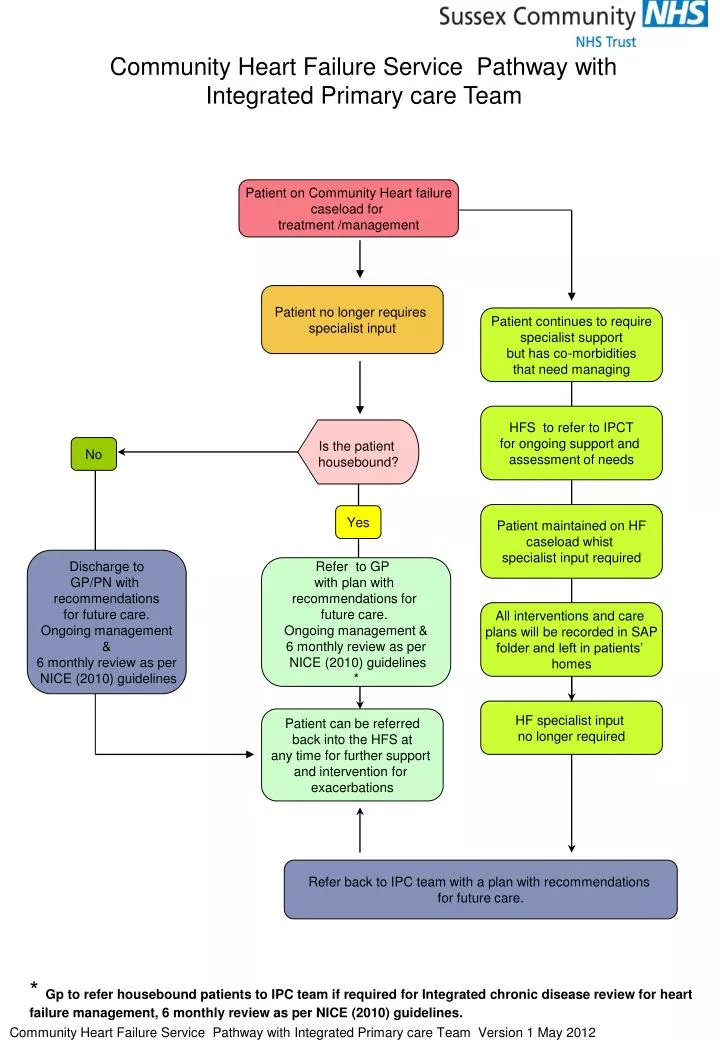
Community Heart Failure Service Pathway with Integrated Primary care Team. Patient on Community Heart failure caseload for treatment /management. Patient no longer requires specialist input. Patient continues to require specialist support but has co-morbidities that need managing.

E N D
Community Heart Failure Service Pathway with Integrated Primary care Team Patient on Community Heart failure caseload for treatment /management Patient no longer requires specialist input Patient continues to require specialist support but has co-morbidities that need managing HFS to refer to IPCT for ongoing support and assessment of needs Is the patient housebound? No Patient maintained on HF caseload whist specialist input required Yes Discharge to GP/PN with recommendations for future care. Ongoing management & 6 monthly review as per NICE (2010) guidelines Refer to GP with plan with recommendations for future care. Ongoing management & 6 monthly review as per NICE (2010) guidelines * All interventions and care plans will be recorded in SAP folder and left in patients’ homes HF specialist input no longer required Patient can be referred back into the HFS at any time for further support and intervention for exacerbations Refer back to IPC team with a plan with recommendations for future care. * Gp to refer housebound patients to IPC team if required for Integrated chronic disease review for heart failure management, 6 monthly review as per NICE (2010) guidelines. Community Heart Failure Service Pathway with Integrated Primary care Team Version 1 May 2012