Download

1 / 35
360 likes | 392 Views
Activity for People with Diabetic Neuropathy. Mamatha Pasnoor , MD Associate Professor Department of Neurology Co-Director, Kansas Neuropathy Center And Patricia Kluding PT PhD Interim Chair & Associate Professor, Physical Therapy and Rehab Science

E N D
Activity for People with Diabetic Neuropathy MamathaPasnoor, MD Associate Professor Department of Neurology Co-Director, Kansas Neuropathy Center And Patricia Kluding PT PhD Interim Chair & Associate Professor, Physical Therapy and Rehab Science Interim Associate Dean for Research, School of Health Professions Associate Director, Clinical and Translational Science Unit University of Kansas Medical Center, Kansas City KS
Diabetic neuropathy • Definition: • Presence of symptoms and/or signs of peripheral nerve, plexus, and/or root dysfunction in people with diabetes • PN affects 2.4 to 7% of the population (JNNP 1997;62:310-318) • CDC National Diabetes Fact Sheet 2011: • 25.8 million diabetics • 60-70% mild to severe neuropathy forms • 35% of U.S. adults aged > 20 years pre-diabetes • 26.4% of diabetic patients have painful neuropathy • The Neuropathy Association estimates > 20 million (6.5%), 50% markedly symptomatic, 150 causes
Pathogenesis • Production of destructive metabolic products: Activation of aldose reductase pathway increased sorbitol levels in nervous tissue • Protein glycation: Glycosylation of nervous tissue structural proteins inactivates and destroys the nervous tissue • Vascular theory: Glucose deposited in basement membrane decreased permeability build up of toxic metabolites.
Classification • Generalized/Symmetric Polyneuropathies • a. Distal Sensory Polyneuropathy (DSPN) • b. Autonomic Neuropathy • c. Diabetic neuropathic cachexia (DNC) • Asymmetric/Focal and Multifocal Diabetic Neuropathies • a. Diabetic lumbosacralradiculoplexopathy • b. Truncal neuropathies (thoracic radiculopathy) • c. Cranial neuropathies • d. Limb mononeuropathies
Diabetic Peripheral Neuropathy is BAD! What is it like to live with neuropathy? • “I feel pins and needles in my feet” • “My pain is severe and 24/7/365. It has taken my joy out of life.” • “My feet are numb and feel dead” • “I’m unsteady when I stand or walk” • “I have open sores on my feet”
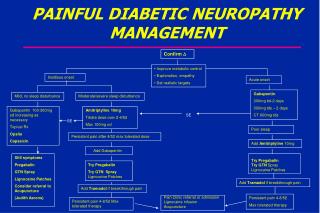
Neuropathic pain management • Treatment of underlying cause • Pharmacological (antidepressant, anticonvulsants, topical agents, analgesics and opiods) • Nonpharmacological • Lifestyle modification, PT & OT (J Diabetes Complications 2012) • Podiatric care & diabetic orthopedic shoes • Pain psychologist & Cognitive Behavioral Rx • TENS • Complementary & alternative medicine: acupuncture, supplements, etc. • Controversial treatments: interventional/regional anesthesia, Anodyne, spinal cord stimulator, peripheral nerve decompression
Background • No proven pharmacologic approaches to reduce DPN risk or slow its progression • Symptom management • Improved glycemic control • Cochrane review (Callaghan, 2012) : • Intensive glycemic control has minimal effect on clinical neuropathy outcomes in people with type 2 diabetes • Physical activity • Improves functional limitations caused by DPN • Promoting peripheral neuroplasticity (Groover, 2013; Kluding, 2012 ; Smith, 2006)
Exercise for DPN: A Paradigm Shift • ADA Standards of Medical Care 2008: “only non-weight bearing activities” in people with DPN • Feet First trial (LeMaster, 2008): RCT in individuals with DPN comparing walking program to control. No increase in foot ulcers.
Is Exercise Effective in DPN?Focus on Function Pain reduction? • Pre-diabetic neuropathy: 1 year diet/exercise counseling, single group (Smith 2006) • DPN: 10 weeks supervised aerobic/resistance exercise, single group (Kluding 2012) • Decrease pain on VAS • DPN: 16 weeks supervised aerobic exercise, single group (Kluding 2015) • No change on BPI-DPN • Decreased pain interference r=-0.4
Is Exercise Effective in DPN?Focus on Function Balance / Fall Risk? • DPN RCT: strength/balance exercise improves balance and reduces fall risk (Allet 2010; Richardson 2001; Song 2011) • DPN RCT: home exercise guided by PT, no effect on balance and fall risk (Kruse 2010)
Activity and Neuropathy • Presence of DPN in older adults associated with decreased activity level as measured by steps per day (van Sloten, 2011) • No studies published investigating the effect of sedentary behavior interventions in people with DPN • No prior randomized controlled studies looking at effect of exercise in diabetic polyneuropathy
Diabetic research • Collaborative effort by three researchers • Douglas Wright, PhD Professor, Anatomy Department • Patricia Kluding, PT, PhD, Associate Professor, Physical Therapy and Rehab Science • Mamatha Pasnoor, MD, Associate Professor, Department of Neurology • Working together since 2006 • Initial project – Epidermal skin innervations in diabetic neuropathy vs CSPN • Pilot project – Safety and efficacy of exercise in diabetic neuropathy
Activity for Diabetic Polyneuropathy: ADAPT • Hypotheesis: • Intervention will • Improve insulin sensitivity • Reduce oxidative stress and inflammation • Enhanced peripheral nerve regenerative capacity • Primary goal • To determine that novel approach to increasing home activity and reduced sedentary time is an effective therapy for DPN
Activity for Diabetic Polyneuropathy: ADAPT • Design: Single blind randomized controlled trial • Methods: • Compare 18 month standard of care to intensive activity intervention • Sites : 2, Utah and Kansas • Total number of subjects to be enrolled=140 • 5 year study
Outcomes • Primary Outcomes (baseline, 9 month, 18 month): • Intraepidermal nerve fiber density ( IENF at distal thigh) • Norfolk Quality of life for diabetic neuropathy (NQOL-DN scale) • Other outcomes • SF-36, VAS pain scale, Brief Pain Inventory, Corneal confocal microscopy, metabolic measures, mood ( Beck Depression Inventory), sleep ( medical outcomes sleep study) scale, Gait analysis (using GaitRite), sudomotor function testing. • Serological testing for metabolic parameters and proinflammatory markers • UTAH specific: Corneal confocal microscopy, muscle biopsy (change in metabolism and intramyocellular lipid), vestibular testing • Biobanking, serum and DNA
Inclusion criteria: Exclusion criteria: Alternative cause of neuropathy History of foot ulcer or amputation Contraindications for skin biopsy, exercise BMI>45 • 30-70 years • Type 2 diabetes • Mild-moderate DPN • Under care of PCP https://pioneersresearch.org/about/active-studies/activity-diabetic-polyneuropathy-adapt-study
Screening visit: CTSU • Consent • Med history / Physical exam • UENS must be 5-18 • NCS • Peroneal • Sural
Screening Visit • Skin biopsy distal leg to confirm neuropathy if NCS is normal • Sudoscan (substudy
Baseline visit: CTSU • Fasting blood draw • DEXA scan: bone density and body composition • Graded maximal exericse test: aerobic fitness / Vo2 max • Distal thigh skin biopsy
RECRUITMENT • Subject enrollment • Neurology clinic database • Neuromuscular clinic database • Pioneers / Frontiers research registry • Cray Center clinic (starting April 2016) • Nov 2015-Mar 2016:
Baseline 2 visit • Gait assessment (10 meter walk, 6 minute walk, Gaitrite) • Fall risk assessment / balance • Questionnaires: 3 day food diary, QOL, pain, depression, sleep, fatigue • 1 week activity monitor
ADAPT INTERVENTION • Standard of Care Intervention Group • 20 minute diet and exercise counseling sessions (baseline & 9 months) • Intensive Intervention Group • Supervised exercise • Home exercise • Sedentary behavior counseling • Dietary counseling
Supervised Exercise • Pre – post exercise assessments • Vital Signs / Blood glucose level • Weekly foot exam • Aerobic exercise • Start 30 min, 50% max heart rate • Resistance exercise • Biceps curl, triceps extension, seated row • Partial squats, hip abduction, heel raises • Balance exercise • Tai Chi
Home Exercise • Teach self assessments • Vitals, blood glucose • Walking 150 min /week • Strength exercises • Level of difficulty customized • Balance exercises • Level of difficulty customized
Sedentary behavior counseling • Motivational interview • Readiness to change • Education about sedentary behavior • Review daily routine, activities at home / work / commute • Home activity monitor with vibrotactile reminders • 7 days • Reminders set every 20 min • Review data in educational session
Dietary Counseling • Core goals: • Proper blood glucose management • Improve body composition • Maintain well-balanced, healthy diet • Nutrition support for physical activity • Nutritional education for type 2 diabetes and DPN • Registered dietician at each site
Dietary Counseling • Session 1 (for example): • Detailed review of 3 day food record • Recommended dietary changes: • Focus on calories, macronutrient distribution, saturated and trans fats, sodium • Weight loss recommendation if appropriate • Encourage daily food tracking • Subject to set 1-3 goals for next visit
Is Exercise Safe? • Sedentary DPN, mean age 58 • N=18 • 16 week supervised aerobic exercise • Improved outcomes (fatigue, aerobic fitness, body composition, sleep quality, vascular) • No change in pain, IENF, neuropathy outcomes • Total of 57 grade 2 AEs (symptoms requiring minimal intervention)
Is neuropathic skin / foot adaptable? • Unless tissue is “dead”, expect positive adaptations from stress (ex) overload • Weight-bearing ex ok for mild deformity but monitor carefully • Integrate activity into lifestyle that works for individual • More research to define parameters of adaptation (Credit Michael Muller PT PhD, Washington University in St Louis)
ADAPT Data Analysis • Aim 1: Compare standard to intensive intervention IENF and QOL outcomes at 18 months • Secondary analyses: 9 month effect; secondary outcomes • Aim 2: Mediation analysis of relationships between change in outcomes
Some unanswered intervention questions… • Is intervention that includes exercise plus sedentary behavior change sustainable in patients with neuropathy? • Which components of the intervention are most effective? • Aerobic, resistance, balance exercises • Sedentary behavior counseling • Nutritional changes • What is the appropriate dosage to accomplish the effect?
ADAPT YEAR 1 ACCOMPLISHMENTS/CHALLENGES • Develop study procedures for 2 sites • IRB reliance agreement • Develop shared REDCap data base • Shipping biopsy/blood samples for central processing • Protocol paper to be submitted to PTJ • Recruitment …
Thanks to … Doug Wright, PhD KUMC ADAPT Team:Jason Rucker PT PhD Linda D’Silva Shaima Alothman Sonia Rawal Constance Bruckner Abdgalghani Yahya Aqeel Alenazi Mohammed Alshehri Nicole Jenci Laura Herbelin Kendra Spaeth Deb Sullivan PhD Angela Cusimano KUMC Neuromuscular Team:MazenDimachkie, Richard Barohn ADAPT Funding: NIDDK 2R01DK064814-09A1 Ziegler Pilot Grant, Dept of Neurology Clinical Pilot / Western States Pilot CTSU Nursing, Exercise Physiology Lab Frontiers/Pioneers Participant Registries