Download
1 / 35
350 likes | 374 Views
Investigating the role of T-regulatory cells in renal ischemic injury, analyzing immune response mechanisms, and exploring treatment strategies. Experimental models, clinical trials, and outcomes are examined.

E N D
T-regulatory Cells in Renal Ischemic injury Alvaro Pacheco-Silva Laboratory of Clinical and Experimental Immunology Division of Nephrology Universidade Federal de São Paulo Hospital do Rim e Hipertensão Hospital Israelita Albert Einstein São Paulo, Brasil
Ischemia and Reperfusion Injury Very complex Incompletely understood Acute Renal Failure (ARF) Delayed Graft Funciton (DGF) Graft Rejection • Ischemic phase - blockade of blood influx, oxygen and nutrients • Reperfusion phase – enhancement of tissue damage • Interaction between vasculature (endothelium), tubular cells and incoming cells. Bonventre & Weinberg, JASN 14:2199-2210, 2003; Schrier et al, J Clin Invest 14(1):5-14, 2004
Oxygen deprivation Reactive oxygen species (ROS) Inflammatory response Haemodynamic events Cellular events Cytoskeletal breakdown Loss of polarity Apoptosis and necrosis Desquamation of viable and necrotic cells Tubular obstruction Endothelial activation Leukocyte activation and migration – neutrophils, lymphocytes, macrophages Cytokines, chemokines Adhesion molecules • Vasoconstriction • Vasodilatation Endothelial and smooth muscle cells structural damage Endothelial-leukocyte adhesion, vascular obstruction Ischemia/Reperfusion Injury
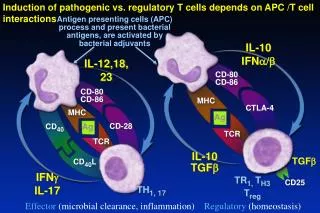
Immune response in IRI Boros and Bromberg, Am J. Transplantation 2005
Impact of ischemia/Reperfusion injury Acute Rejection Renal Fibrosis P 0,01 45 NO DGF 40 With DGF 35 30 P 0,01 25 Rejection (%) 20 15 10 5 0 6 months > 6 months Discharge Ojo et al. Transplantation 1997. Burne-Tarne al. Kidney Int 2005.
Prediction of Clinical outcomes (DGF) Variables p value Donor type <0,001 CIT 0,005 WIT 0,013 TNFα <0,001 CD25 <0,001 TGF-β<0,001 A20 <0,001 IL-10 <0,001 ICAM 0,006
CD4+T lymphocytes and IRI A phase I trial of immunossupression with anti-ICAM-1 (CD54) mAb in renal allograft recipients. Haug C. et al. Transplantation 55(4):766-772, 1993. N= 18 hight risk for delayed graft function patients Follow up 16 to 30 months
Fig. 1 Fig. 2 Post Op Days CD4+T lymphocytes and IRI A prospective, randomized, clinical trial of intraoperative versus postoperative Thymoglobulin in adult cadaveric renal transplant recipients. Goggins WC. et al.Transplantation. 76(5):798-802, 2003
b a CD4 -/- WT type WT type Nu/nu mice Nu/nu mice reconstituted wild-type T cells CD4-/- reconstituted with wild-type T cells CD4+T lymphocytes participates on IR injury Identification of the CD4+T cell as a major pathogenic factor in ischemia acute renal failure. Burne MJ. Et al. J Clin Invest. 2001 Nov;108(9):1283-90.
PROTECTIVE MECHANISMS INJURY Strategies of treatment IRI
Tregs and Innate immune response Enhanced Regulatory T Cell Activity is an Element od the Host response to Injury Choileain NN. Et al. J immunol 2006 Jan 1;176(1):225-36
Regulatory T cells Adaptative T regs: Induced from naive T cells by antigenic stimulation and cytokine millieu IL-10(Roncarolo et al, 2006) TGF-beta(Nakamura et al, 2004) Developmental classification for T Reg Naturally arising T reg cells: Constitutive expression at higher levels: Interleukin (IL)-2 receptor alpha chain (CD25) (Sakaguchi et al., 2004) CTLA-4 (CD152) (Sakaguchi et al., 2004) Glucocorticoid induced TNF receptor (GITR) (McHugh et al., 2002, Shimizu et al., 2002) FOXP3(Schubert and Ziegler et al, 2001, Fontenot et al, 2003; Hori et al, 2003)
CD4+ T cells Post ischemic injury CD4+CD25+Foxp3+ T Cells Post ischemic injury CD4+ effector T Cells Decrease number (Anti-CD25 depleting antibody) ? Increase CD4+ effector T cells activity Decrease suppressor activity (Anti-GITR) CD4+T lymphocytes in Renal Ischemia reperfusion modelStrategies
PC61: depleting rat IgG1 anti-CD25 (alpha chain of IL-2R) Choileain NN. Et al J. Immunol, 2006
DTA-1: agonist rat IgG2a anti-GITR (Glucocorticoid-induced TNF receptor) DTA-1 mAb abrogates suppression mediated by CD25+CD4+ T cells breaking immunological self- tolerance
DTA-1 mAb abrogates suppression mediated by CD25+CD4+ T cells leading to development of autoimmune gastritis in mice
Sacrifice: Blood, kidneys, spleen, lymph nodes harvested Treatment PC61 200 g DTA-1 400 g IgG 400 g Isquemia 45 min Day 2 (24 hs) Day 1 Day 0 Day 4 (72hs) IR antibody treatment Protocol
Background: C57 BL/6 male cm Microclamps for renal artery and vein (renal pedicle) IRI model adapted from KELLY et al., 1996 Renal Ischemia Reperfusion Model Reperfusion times : 24 and 72hs Analyses: blood: creatinine and urea LN, spleen: flow cytometry Kidneys: morphometry, Real Time PCR
IR antibody treatment Effect of Antibody treatment in TCD4+CTLA4+Foxp3+ cells PC61 Treatment DTA-1 Treatment
IgG PC61 IR 24 PC61 IR 72 12.62 18.22 Spleen 10.52 3.11 1.57 8.08 pRenal LN IR antibody treatment Depletion of TCD4+CTLA4+Foxp3+ cells
P=0,0002 P=0,0018 P=0,0033 P=0,0001 IR antibody treatment Renal Function Outcome
* * * Morphometric analyses Acute tubular necrosis and tubular regeneration IR 24 hours * p< 0.001
* * * Morphometric analyses Acute tubular necrosis and tubular regeneration IR 72 hours * p< 0.001
A C B Sham IgG DTA-1 400 mg PC61 200 mg D 24 H H F G E 72 H IR antibody treatment Histopathological analyses HE I Kidney Tissue HE. A, B, C, D: IR 24 hs. A: Sham, B: IgG treated, 400 micrograms C: PC61 treated, 200 micrograms. D: DTA-1 treated, 400 micrograms, E, F, G, H: IR 72 hs. E: Sham, F: IgG treated, 400 micrograms, G: PC61 treated 200 micrograms mg, H: DTA-1 treated, 400 microgams.
IR antibody treatment Anti-Inflammatory Genes/TH2 response
IR antibody treatment Pro-Inflammatory Genes
IR antibody treatment Conclusions and Perspectives At 24 hours of reperfusion, depletion of TCD4+CTLA-4+Foxp3+ cells was 30,3% (spleen) and 67,8% (para renal lymphnodes).After 72 hours of reperfusion, depletion of TCD4+CTLA-4+Foxp3+ was 43,1% (spleen) and 90,22% (para renal lymphnodes). This depletion was efficient in generate significant responses in both 24 hours and 72 hours if reperfusion Depleted mice presented similar renal function to control animals at 24 hours, but 72 hours after IRI, PC61 treated mice presented significant worst renal function compared to the group that received IgG. DTA-1 treated animals presented significant protection at the same timepoint, indicating that different subsets of cells can be acting at these timepoints. Furthermore, histopathological analyses showed that there was a pronounced incidence of necrosis for both PC61 treated and IgG in IR 24 hours experiments. On the other hand, in IR 72 hours experiments we observed a regeneration pattern in both PC61 and IgG treated animals, but in the PC61 treated group there was a significant necrosis index (p<0.001), comparing with IgG treated group, suggesting that TCD4+CTLA4+FOXP3+ cell population could be important in a late phase of injury recover. It is known that the stress and tissue damage associated with IRI influence the development of a immune response to protect the tissue damage. Thus, our results suggests a role for TCD4+CTLA4+FOXP3+ cells (naturally arising T teg cells) in renal IRI experimental model.
CD4+CD25+Foxp3+ T Cells Post ischemic injury CD4+ effector T Cells 24 hs: TCD4+ effector Stimulated by DTA-1 escape from T Reg suppression and make injury worst Proinflamatory cytokines IL-1b and IL-6 Anti inflamatory genes Such as HO-1 and polarization toward Th2 (GATA-3) transcription factor 72 hs: If there is no T Reg at this point (PC61 treatment), there is no recovery from injury Persistence of necrosis IR antibody treatment Hypothesis 72 hs: TRegs GITRhigh stimulated by DTA-1 start to suppress TCD4+ response
IR antibody treatment Perspectives
Acknowledgements Rebecca M. M. Monteiro Marcio J. Damião Giselle Gonçalves Carla Q. Feitoza Marcos Cenedeze Nephrology Division - Universidade Federal de São Paulo Brazil Prof. Dr.Mauricio M. Rodrigues Fanny Tzelepis Interdisciplinary Center for Gene Therapy CINTERGEN Universidade Federal de São Paulo, Brazil Prof. Dr.Niels Olsen S. Camara Immunology Division Universidade de São Paulo USP, Brazil Vicente de Paula A. Teixeira Marlene A. dos Reis Department of Pathology, Universidade Federal de Uberaba, Minas Gerais, Brazil Prof Dr. S. Sakaguchi T. Yamaguchi (DTA-1) H. Uryu (PC61) K. Nagahama (IRI) M. Ono (Real Time PCR) Institute for Frontier Medical Sciences Kyoto University Japan