Download
1 / 12
120 likes | 412 Views
STOMACH AND DUODENUM. Chapter 13. STOMACH AND DUODENUM Objectives. Anatomy and Physiology Peptic Ulcer Disease Zollinger Ellison Syndrome Neoplasms. Anatomy STOMACH. Four regions Cardia, Fundus, Antrum, Pylorus Parietal cells, Chief cells, Antral G cells, Mast cells Blood supply

E N D
STOMACH AND DUODENUM Chapter 13
STOMACH AND DUODENUMObjectives • Anatomy and Physiology • Peptic Ulcer Disease • Zollinger Ellison Syndrome • Neoplasms
AnatomySTOMACH • Four regions • Cardia, Fundus, Antrum, Pylorus • Parietal cells, Chief cells, Antral G cells, Mast cells • Blood supply • Gastric and gastroepiploic arteries • short gastrics and gastroduodenal • Innervation • Vagus
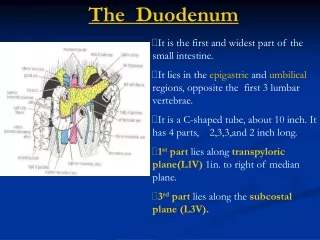
AnatomyDUODENUM • Four regions • Bulb, Descending, Transverse, Ascending • Blood supply • Mainly from gastroduodenal artery
Physiology • Acid Secretion • Parietal Cell • acetylcholine, gastrin, histamine • Cephalic phase- sight/smell, vagal • Gastric phase- antral distention, gastrin • Intestinal phase- histamine • Inhibition of gastric acid • Secretin • Somatostatin
Acute Ulcer Disease • Most common in 1st portion of duodenum and lesser curvature of the stomach • Burning epigastric pain • Duodenum- relieved by food • Stomach- produced by food • Upper GI bleed • Acute abdomen • gastric outlet obstruction • Diagnosis • history • Upper GI series • Endoscopy
Acute Ulcer DiseaseTreatment • Upper GI Bleed • NGT, Large IV’s, Resuscitation, antacids/H2 Blockers, Endoscopy • Surgery- if > 6 U of blood or if remains unstable • Perforation- Exp Lap • Graham’s patch • Acid reducing procedure • Gastric outlet obstruction • NGT, IVF, Correct electrolyte abnormalities • Surgical inervention if necessary
Chronic UlcerTreatment • Conservative medical treatment • Diet- avoid caffeine, alcohol, chocolate • H2 blockers • Proton pump inhibitors • H. Pylori eradication- 2 weeks of triple therapy • Surgical • Truncal vagotomy and pyloroplasty • Selective vagotomy and pyloroplasty • Proximal gastric vagotomy • Antrectomy- Billroth I and II • For gastric ulcers be suspicious for cancer
Zollinger Ellison Syndrome • Gastrinoma- gastrin producing tumor • 60% are malignant- slow growth pattern • Associated with MENS I • Present with refractory PUD. • Diagnosis- • fasting gastrin serum >300 • Secretin infusion test • Treatment • Medical • Surgical excision
Gastric Carcinoma • Epidemiology- Geographic and diet • Presentation- Usually Asx. • Bloating, wt loss, melena, + hemoccult • Pathophysiology • All gastric CA are adenocarcinomas • Polypoid, ulcerating, linitis plastica • Metastasis through lymph nodes • Diagnosis • Upper GI Series • Endoscopy andbiopsy • CT Scan
Gastric Carcinoma • Treatment • Surgical Resection- subtotal gastrectomy and gastrojejunostomy vs. total gastrectomy • 5 year survival of 10% • Palliation • Chemoradiation- no survival benefit