Download
1 / 1
10 likes | 145 Views
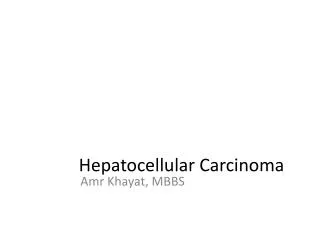
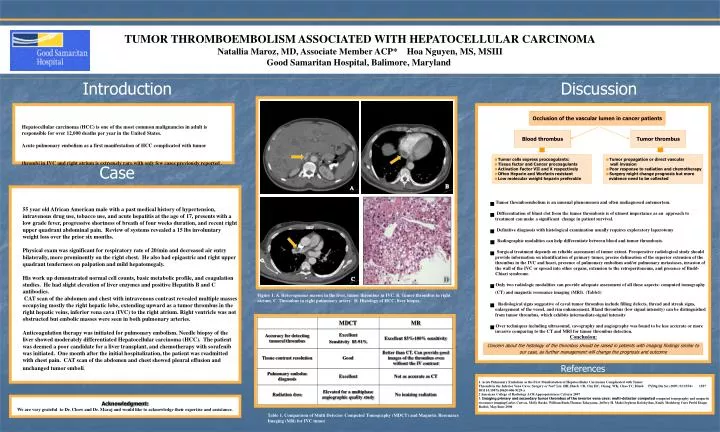
B. A. C. D. TUMOR THROMBOEMBOLISM ASSOCIATED WITH HEPATOCELLULAR CARCINOMA Natallia Maroz, MD, Associate Member ACP* Hoa Nguyen, MS, MSIII Good Samaritan Hospital, Balimore, Maryland. Introduction. Discussion.

E N D
B A C D TUMOR THROMBOEMBOLISM ASSOCIATED WITH HEPATOCELLULAR CARCINOMA Natallia Maroz, MD, Associate Member ACP* Hoa Nguyen, MS, MSIIIGood Samaritan Hospital, Balimore, Maryland Introduction Discussion Hepatocellular carcinoma (HCC) is one of the most common malignancies in adult is responsible for over 12,000 deaths per year in the United States. Acute pulmonary embolism as a first manifestation of HCC complicated with tumor thrombi in IVC and right atrium is extremely rare with only few cases previously reported . • Tumor thromboembolism is an unusual phenomenon and often undiagnosed antemortem. • Differentiation of blunt clot from the tumor thrombosis is of utmost importance as an approach to treatment can make a significant change in patient survival. • Definitive diagnosis with histological examination usually requires exploratory laparotomy • Radiographic modalities can help differentiate between blood and tumor thrombosis. • Surgical treatment depends on reliable assessment of tumor extent. Preoperative radiological study should provide information on identification of primary tumor, precise delineation of the superior extension of the thrombus in the IVC and heart, presence of pulmonary embolism and/or pulmonary metastases, invasion of the wall of the IVC or spread into other organs, extension to the retroperitoneum, and presence of Budd-Chiari syndrome. • Only two radiologic modalities can provide adequate assessment of all these aspects: computed tomography (CT) and magnetic resonance imaging (MRI). (Table1) • Radiological signs suggestive of caval tumor thrombus include filling defects, thread and streak signs, enlargement of the vessel, and rim enhancement. Bland thrombus (low signal intensity) can be distinguished from tumor thrombus, which exhibits intermediate-signal intensity • Over techniques including ultrasound, cavography and angiography was found to be less accurate or more invasive comparing to the CT and MRI for tumor thrombus detection. Conclusion: Occlusion of the vascular lumen in cancer patients Blood thrombus Tumor thrombus • Tumor cells express procoagulants: • Tissue factor and Cancer procoagulants • Activation Factor VII and X respectively • Often Heparin and Worfarin resistant • Low molecular weight heparin preferable • Tumor propagation or direct vascular • wall invasion • Poor response to radiation and chemotherapy • Surgery might change prognosis but more evidence need to be collected Case • 55 year old African American male with a past medical history of hypertension, intravenous drug use, tobacco use, and acute hepatitis at the age of 17, presents with a low grade fever, progressive shortness of breath of four weeks duration, and recent right upper quadrant abdominal pain. Review of systems revealed a 15 lbs involuntary weight loss over the prior six months. • Physical exam was significant for respiratory rate of 20/min and decreased air entry bilaterally, more prominently on the right chest. He also had epigastric and right upper quadrant tenderness on palpation and mild hepatomegaly. • His work up demonstrated normal cell counts, basic metabolic profile, and coagulation studies. He had slight elevation of liver enzymes and positive Hepatitis B and C antibodies. • CAT scan of the abdomen and chest with intravenous contrast revealed multiple masses occupying mostly the right hepatic lobe, extending upward as a tumor thrombus in the right hepatic veins, inferior vena cava (IVC) to the right atrium. Right ventricle was not obstructed but embolic masses were seen in both pulmonary arteries. • Anticoagulation therapy was initiated for pulmonary embolism. Needle biopsy of the liver showed moderately differentiated Hepatocellular carcinoma (HCC). The patient was deemed a poor candidate for a liver transplant, and chemotherapy with sorafenib was initiated. One month after the initial hospitalization, the patient was readmitted with chest pain. CAT scan of the abdomen and chest showed pleural effusion and unchanged tumor emboli. Figure 1. A. Heterogonous masses in the liver, tumor thrombus in IVC. B. Tumor thrombus in right atrium. C. Thrombus in right pulmonary artery. D. Histology of HCC, liver biopsy. Concern about the histology of the thrombus should be raised in patients with imaging findings similar to our case, as further management will change the prognosis and outcome References 1. Acute Pulmonary Embolism as the First Manifestation of Hepatocellular Carcinoma Complicated with Tumor Thrombi in the Inferior Vena Cava: Surgery or Not? Lin HH, Hsieh CB, Chu HC, Chang WK, Chao YC, Hsieh TYDig Dis Sci (2007) 52:1554– 1557 DOI 10.1007/s10620-006-9129-x 2 American College of Radiology ACR Appropriateness Criteria 2007 3. Imaging primary and secondary tumor thrombus of the inverior vena cava: multi-detector computed computed tomography and magnetic resonance imagingCarlos Cuevas, Molly Raske, William Bush,Thomas Takayama, Jeffrey H. Maki,Orpheus Kolokythas, Emily Meshberg Curr Probl Diagn Radiol, May/June 2006 Acknowledgment: We are very grateful to Dr. Chow and Dr. Maraj and would like to acknowledge their expertise and assistance. Table 1. Comparison of Multi Detector Computed Tomography (MDCT) and Magnetic Resonance Imaging (MR) for IVC tumor