Download
1 / 17
180 likes | 404 Views
Case report of an Oesophageal Leiomyosarcoma. Dr Lukram Ajit Singh Dr Kalyan Kar Dr Gautam Mukhopadhyay Dr M B Das Dept Of Oncosurgery and Oncology. Background

E N D
Case report of an Oesophageal Leiomyosarcoma Dr Lukram Ajit Singh Dr KalyanKar Dr GautamMukhopadhyay Dr M B Das Dept Of Oncosurgery and Oncology
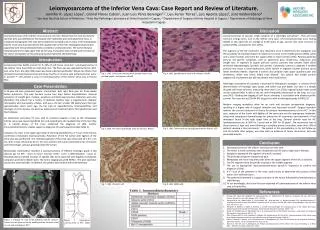
Background Leiomyosarcomas of the oesophagus are rare tumours first describedalmost 100 years ago. They are malignant tumours that originatefrom smooth muscle cells that may be difficult to differentiatefrom the benign tumours leiomyomas, especially if they are well-differentiated.The tumours typically have a slow rate of growth that may furtherlure the surgeon into a false diagnosis. Leiomyosarcomas accountfor 5% of gastrointestinal and 0.5% of all oesophageal sarcomas.In most instances dysphagia and odynophagia are the commonestpresenting symptoms .
Leiomyosarcoma is a high-graded, smooth muscle tumor of mesenchymal origin that can arise in the gastrointestinal tract. In esophagus, it is rare, only accounting for less than 1% of malignant tumor. Diagnosis is based on pathologic and immunohistochemical findings. Because of its location in the submucosal layer, it usually grows to a huge mass by the time symptoms appears
Our Case Report: • Mr. SD a 45 years old gentleman , a resident of Siliguri and a business man by profession was referred to our Surgery Department with presenting complaints of: • 1. Difficulty in swallowing both liquids and solid foods for last 8 months. The complaint had worsen recently and he was unable to eat solids but was able to drink water with some effort. • 2. Loss of weight from a good 68 kilos to 55 kilos on presentation. • 3. Pallor
Work up: • Routine blood: On admission(19th Oct ‘10) • Hb: 8.3% • PCV: 24.9% • TC: 9900 • Na: 137 • K :2.7 • Coagulation profile: WNL
As is seen from the blood report on admission, patient was anemic and was having electrolyte imbalance from days of starvation. • He had already undergone CT scan of the thorax, Upper GI Endoscopy and biopsy of the oesophageal lesion.
CT Report: Evidence of a large elongated endoluminal heterogenously enhancing soft tissue density with smooth margins arising from left lateral wall of the oesophagus extending superiorly to subcarinal region and inferiorly upto gastro esophageal junction. There is near obliteration of the oesophageal lumen by the lesion. The lesion measures 6 x 2.9 x 14.6 cm in size. No enlarged Lymph nodes are seen in the mediastinum. Impression is of a neoplastic condition such as leiomyoma or any other pathology.
Upper GI Endoscopy: • Big 13cm/7mm/5mm mucosal and sub mucosal growth of middle and lower third of oesophagus with some degree of obstruction at this point. • Impression ?? Sub mucosal leiomyoma vs others.
Plan for Oesophagectomy: • Correction of blood abnormalities and electrolyte imbalance. • Fitness for surgery • Team consisting of an Onco Surgeon, a Cardiothoracic Surgeon, a General Surgeon , Anaesthetist and a Physician decided on the planned procedure and Mr SD was put up for surgery on the 25th Oct ‘10.
IVOR LEWIS PROCEDURE • Abdominal Part: Midline incision. Lesser sac opened. Mobilisation of stomach. Division of cardia from lower end of oesophagus. Cardia closed and fixed to lower of oesophagus to be pulled up through the hiatus via the thoracic incision. • Thoracic Part: Lateral thoracic incision through 5th intercostal space on the right side of chest. Right lung was made to collapse by only left lung ventilation.
Dissection of oesophagus and oesophagus divided in the upper middle part. Lower end of oesophagus pulled up with cardia of stomach attached to it. Delivery of specimen- oesophagus with the growth. Anastomosis of oesophagus with the pulled up stomach in 2 layers with vicryl. A drain was placed in the right thoracic cavity. • Feeding Jejunostomy. • Closure.
Final Report of Contrast Swallow: • Water soluble oral contrast shows smooth transit though distal gastric tract without any obvious hold up or extravasation in thorax. • No abnormal mediastinal collection noted.
Histopathological report: • High grade leiomyosarcoma of the oesophagus. • Surgical resection margins are free of tumour.
Conclusion: The CT features of leiomyosarcoma is non-specific. It usually appears as a large mass with frequent areas of cystic and myxoid degeneration; while, calcification is rather uncommon. These features can be easily confused with neural or other neoplasm. Therefore, imaging modalities are not enough for definitive diagnosis and usually requires definite histopathologic analysis