Download
1 / 21
210 likes | 401 Views
Genetic Research in Dementia: Risk Evaluation & Education for Alzheimer’s Disease. Supported by grants from: National Human Genome Research Institute (ELSI) HG/AG-02213 (The REVEAL Study); National Institute on Aging AG-09029 (The MIRAGE Study) and AG-13846 (BU Alzheimer’s Disease Center).

E N D
Genetic Research in Dementia:Risk Evaluation & Education for Alzheimer’s Disease Supported by grants from: National Human Genome Research Institute (ELSI) HG/AG-02213 (The REVEAL Study); National Institute on Aging AG-09029 (The MIRAGE Study) and AG-13846 (BU Alzheimer’s Disease Center) Scott Roberts, PhD1 Robert C. Green, MD, MPH1,2 Departments of Neurology1 and Medicine2 (Genetics Program) Alzheimer’s Disease Center Boston University School of Medicine
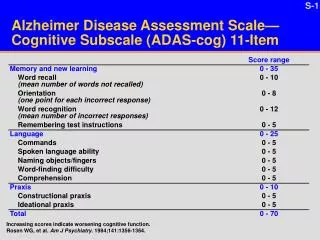
Alzheimer’s Disease & Public Health • AD is the most common cause of dementia among people age 65 and older. • An estimated 4.5 million in the US currently have AD. • Annual costs estimated at $100 billion • High caregiver burden (“death by a thousand subtractions”) • By 2050, 13.2 million older Americans are expected to have AD if current demographic trends continue and no preventive treatments become available. Source: NIA’s “Alzheimer's Disease: Unraveling the Mystery.”
Established Gene Markers for AD Deterministic Mutations: Amyloid Precursor Protein (APP) Presenilin-1 (PS-1) Presenilin-2 (PS-2) Susceptibility Polymorphism: Apolipoprotein E (APOE) Lendon CL, et al. JAMA 1997;277(10):825-831
APOE Genotyping for Risk Assessment Why should we NOT do risk assessment for Alzheimer’s disease (at least with APOE)? • APOE genotype is not a highly accurate marker • No progression/prevention intervention available • Discrimination or psychological harm may occur • Five negative consensus recommendations
APOE Genotyping for Risk Assessment Why SHOULD we do risk assessment for Alzheimer’s disease (using APOE)? • Define at-risk populations for prevention trials • Identify responsive subgroups • Respond to clinical requests • Develop new “clinical technologies” for • susceptibility markers in common disorders
“I don’t skate where the puck is. I skate to where it’s going.” - Hockey superstar Wayne Gretzky
Risk Evaluation & Education for AD (The REVEAL Study) An Intervention Trial where Information is the Intervention: What is the impact of genetic risk assessment for adult children of people with AD?
Key Questions Who wants to know? What happens to them? What do they do?
Study Protocol Enrollment Education Blood Draw and Randomization Risk Disclosure and Counseling using family hx, gender, APOE Risk Disclosure and Counseling using family hx, gender alone Follow up (6 weeks, 6 months, 12 months)
Baseline Demographics by Randomization Group Demographic Characteristic Control (N = 51) Intervention (N = 111) 52.0 (10.0); 30-76 55.3 (9.0); 37-78 Mean Age, yrs. (SD); Range Sex, % female 69.4% 78.4% 90.2% Race/ethnicity, % White 95.5% 16.7 (2.2); 12-22 Mean yrs of education (SD); Range 16.8 (2.5); 10-22 Marital status, % married 66.7% 60.8% No. of affected relatives, % 1 2+ 40.5% 59.5% 45.1% 54.9% Median income bracket $70K-$99,999 $70K-$99,999
Who Wants Genetic Risk Assessment? • 24% of systematically contacted research registry participants enrolled in the RCT • 80% of Education Session attendees subsequently proceeded to randomization • Age (younger), education (higher), and gender (female) predicted RCT enrollment Roberts et al., Genetics in Medicine, 2004
Test Uptake Across Diseases Roberts et al., Genetics in Medicine, 2004
Reasons Associated with Test Uptake Women strongly endorsed more reasons for seeking testing than men, p = .01 Roberts et al., ADAD, 2003
Mean Depression Scores Clinically significant depression
Mean Anxiety Scale Scores Clinically significant anxiety
Mean Impact of Event Scale Scores Clinically significant impact
Changes in Health Behaviors e4+ group > e4- group, p < .05 Most common changes: Adding vitamins (48%) Changing diet (13%) Exercise (6%)
Insurance Changes Reported at 12 Month Follow-Up * Zick, Mathews, Roberts et al., Health Affairs, 2005
Conclusions • Genetic risk assessment will become increasingly important part of medical care • Alzheimer’s disease and APOE represent an instructive paradigm • Need to develop empirically validated methods of disclosing genetic risk information
Boston University Robert C. Green, MD, MPH Tamsen Brown, MS, CGC Dapo Akinleye, MPH Lindsay A. Farrer, PhD L. Adrienne Cupples, PhD George Annas, JD, MPH Weill Medical College/Cornell Univ. Norman R. Relkin, MD, PhD Lisa Ravdin, PhD Susan LaRusse, MS, CGC Beth Chisholm, MS Elana Cox, MS, CGC Howard University Charmaine Royal, PhD Thomas Obesisan, MD Grace-Ann Fasaye, ScM Case University Peter Whitehouse, MD, PhD Eric Juengst, PhD Melissa J. Barber, ScM Stephen Post, PhD Indiana University Kimberly A. Quaid, PhD University of British Columbia A. Dessa Sadovnick, PhD King’s College, London Theresa Marteau, PhD Nat’l Human Genome Research Inst. Barbara Biesecker, MS Elizabeth Thomson, MS, RN Duke University Robert Cook-Deegan, MD Acknowledgments/Investigators