Download

1 / 22
230 likes | 381 Views
Compliance Support & DDA. A number of Anecdotes!. DDA applies to. People with a mental, sensory or physical impairment that has a substantial and long-term adverse effect on their ability to carry out normal day-to-day activities

E N D
Compliance Support & DDA A number of Anecdotes!
DDA applies to People with a mental, sensory or physical impairment that has a substantial and long-term adverse effect on their ability to carry out normal day-to-day activities (no longer necessary for the mental impairment to be clinically recognised)
What does this mean? Substantial – has an impact on day to day tasks Long-term – lasts at least a year or for the rest of the person’s life
Substantial A person would be considered as having a disability only if the impairment has a substantial effect on the person’s ability to carry out normal day to day activities
Impairment Must impact on at least one of: • Mobility • Manual dexterity • Physical co-ordination • Speech, hearing, eyesight • Memory • Ability to concentrate, learn or understand • Continence • Ability to lift, carry or move everyday objects • Understand the risk of physical danger BUT – there is no definitive list ………..
Support for people with disabilities • All service providers have to make “reasonable adjustments” • No service provider can be directed to make a specific adjustment • Does not include supporting carers who are not insured to ‘give’ medicines
Where to start…. • It’s a minefield! • The Collaborative’s work has been involved predominantly with one pharmacist and his Monitored Dosage System (MDS) domiciliary patients – and a PCT led initiative to asses the size of the problem • The LPC has also been involved in large project in this area
The Mid Devon Experience! • Pharmacy Forum held in December to discuss an LES in compliance support • All pharmacists re-assessed their base line number of patients on MDS • Over a considerable period of time the assessments forms were submitted for further work
The Neil Ansell Experience! • Large number of patient on MDS • Prior to the forum, consulted the GPs and told them he was inundated with MDS and could not cope. Surgery agreed to think before recommending patients for MDS • Forum made position very clear for Neil – visited and assessed his pre existing 42 patients, with both an MUR and the Devon Concordance Tool. • Neil and Collaborative worked together on a measuring sheet to see if the reassessment improved the patient experience (included in your packs)
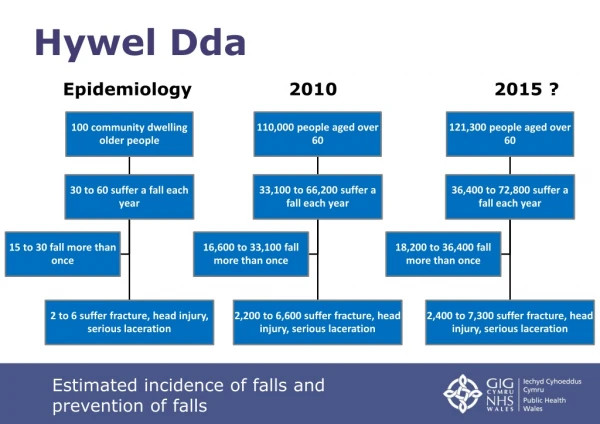
The Results!!! *Some with diagnosed conditions, but since Dec 2005 very difficult to ascertain this criteria. 31 MDS patients out of 42 were Disabled under the meaning of the Act They were disabled in the above categories
Some more facts! • The 11 patients not DDA all had carers (family/paid carers) - majority of which did not understand the medication of their relatives / clients • Assessment took 45 minutes per person, mostly after work, or if a locum cover available 3 per day. • Of the entire 42 original patients, only 5 regularly came into the shop
The Next Steps • The agreement is now when GP’s phone the pharmacy and request an MDS, Neil makes it clear he will carry out the assessment and make the decision himself.
Some Problems! • Customer demand their medicines be put in a tray, as OT said this could be done for free in chemist. • Work with and re-educate other healthcare providers e.g. district nurses and Occupational Therapists about this situation. Find out from your local PCT who the leads are.
Current Situation • Since the re-assessment 6 new requests for MDS – from patients / carers / surgery requests. • Carried out an assessment – started them all with medicine reminder chart with a review after 1 month. • Only 1 had a blister pack after this initial period but deteriorated very quickly and went into a nursing home. • This proves that pharmacy judgement and worth in the community. • If they still insist on having a tray Neil gave them an over the counter simple medicines tray if this is better for the carers confidence in administering medicines.
Torbay Assessments • 2004 Survey to establish baseline usage of community based patients • Devon LPC Torbay tPCT Joint Project • Concordance survey • Assessment tools tested
LPC Project - Main findings • 432 patients in the community • 57 assessments – 20% fell outside DDA • MDS appropriate in less than one third of all patients assessed • Eight MDS initiated in secondary care, one patient appropriate • Identification of patient group outside DDA who would benefit from support
How do you know? The assessment process – 3 steps • Identify factors that affect the patients ability to take their medicines • Identify what adjustment would enable the person to take their medicines • Identify whether ‘DDA’ applies
Outcomes Sight – can you read the instructions on the label? A reasonable adjustment might be • A pictogram • Large font • RNIB bump ons An unreasonable adjustment might be • Making an adjustment if the patient does not have corrective spectacles
Outcomes Manual Dexterity – Do you have problems getting medicines out of their bottles or popping medicines out of blister packaging? A reasonable adjustment might be • Supply of larger than needed bottles or easy to open caps, winged lids • De-blistering of medicines or the free provision of a de-blister device An unreasonable adjustment might be • The provision of medicine in a compliance aid that the person is unable to self manage
Outcomes Mobility – Do you have problems getting a regular supply of your medicines? A reasonable adjustment might be • Free collection and delivery service even if the service is offered to other patients at a small charge An unreasonable adjustment might be • The introduction of a collection and delivery service if one is not in place, or extending the collection and delivery area to an unreasonable distance
Lessons learnt so far • Link to Medicines Use Review • Approach the assessment like a structured consultation • Develop communication skills and TIME management • Engage other members of the health and social care team - TALK • Investigate opportunities under practice based commissioning • MDS is not always the answer!
Useful websites • www.psnc.org.uk • www.primarycarecontracting.nhs.uk • www.pjonline.com • www.drc-gb.org (Disability Rights Commission) • www.npa.co.uk • www.opsi.gov.uk/acts/acts1995/Ukpga_1995050_en_1.htm (Disability Discrimination Act)