Download
1 / 16
160 likes | 257 Views
WestawayGillis Innovators in Healthcare Solutions. Development of a Business case in the NHS Mr Kim Sergeant Managing Director. Agenda. Context – the NHS today Focus on PCTs Business cases Information needs Good business cases Common mistakes.

E N D
WestawayGillisInnovators in Healthcare Solutions Development of a Business case in the NHS Mr Kim Sergeant Managing Director
Agenda • Context – the NHS today • Focus on PCTs • Business cases • Information needs • Good business cases • Common mistakes
Although NHS Trusts remain the main providers of secondary care…they now get their money from PCTs! Department of Health Accountability Contracts Budgets Own org money only PCTs hold 75% of the NHS budget! 28 SHAs ‘Special payments’ 308 PCTs & CTs Acute Trusts & Foundation Trusts Local Authorities
PCTs are responsible for commissioning the majority of care… Central commissioning PCT PCT Consortia at different levels • Board sets overall strategy • Executive (PEC) develops policy Primary Mental health Secondary Specialised GMS GPs PMS GPs & PMS Plus “Provider services” employed by PCTe.g. District Nurses, Health Visitors Mental Health Trusts NHS Trusts Private Sector Tertiary & specialist centres
From a Trust perspective things are changing too… Historically • Trusts hold contracts with multiple commissioners • Commissioning arrangements are often based on historical precedent and do not change frequently • Some localities have block contracts, others have case-by-case arrangements • Contracts may or may not include cost of drugs
Introduction of Payment by Results– HRGs & the National Tariff • The new system of payment will be introduced gradually over five years • HRGs and a national tariff will be put in place to enable volume-casemix commissioning • This will be developed to capture as much NHS activity as possible, so radically changing PCT commissioning methods • Foundation Trusts will use the National Tariff for all procedures from April 2004
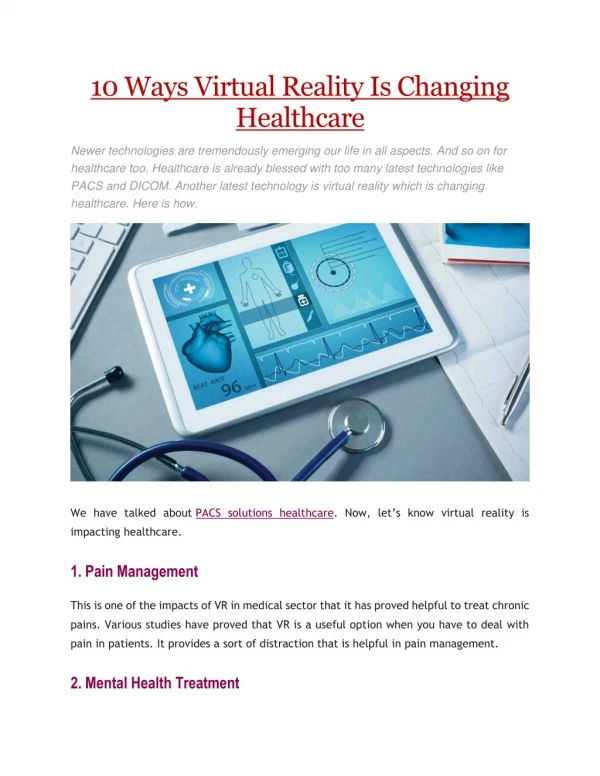
Across the NHS there is an increasing need to justify new or increased investment in services or products • Key questions to address include: • What is the product / service • New drug / indication / technique • The problem / situation this is addressing • The benefits • Where will it be prescribed / utilised • Who will it be prescribed to / used for (specific groups of patients / entry and exit criteria) • Performance in relation to alternative therapies / techniques • Efficacy • Safety • Where does it fit with national / local priorities
Even if D&T Committee approval is given funding still needs to be found • Funding can be found by • Using within current budget • replacement / cheaper products • stopping doing something else • Approach the Trust for funding • Approach PCT for in-year funding • Approach PCT for future funding
Timing is important for success:thefunding process starts in September • 2º care directorates look at previous spend • Budgeted figure • Outturn • Within directorates each department will review • future requirements • Cost pressures • Review inflationary uplift and any savings that may be needed
2º Care Business / directorate manager Management accountant Chief pharmacist / directorate senior pharmacist Clinician Contract manager dealing with commissioners Director of operations 1º Care / PCT Director of Commissioning / Lead commissioner Chief pharmacist Chair of Rx committee Finance Director There are key stakeholders involved in the process
Within the trust – priorities have to be established Each directorate flags up budget needs Trust management team Prioritisation process starts Agreement reached in funding - LDP Trust meet with PCTs
Money will generally follow priority areas • Anything that can demonstrate a positive impact on • waiting lists • waiting times • Star ratings • Anything that fits in with the PCT priorities
When presenting a ‘business case’ PCTs have specific information needs • Impact on other parts of the system • Primary/secondary care interface • Walk in centres • PGDs (Patient Group Directives) • Nurse/pharmacist prescribing • training • Policy/target hooks/performance management • Any impact on NICE/NSFs • “This is the bit that the industry are pretty good at” • Costs – in a form that matches up with requirements and reflects NHS budgeting & planning frameworks • Immediate costs • Longer term costs
If the case isn’t clear cut additional information may be requested • Effect on referrals • “Likely to become more critical under new contract as GPs already feel over-burdened” • Risks andassumptions in realising financial benefits • Are there external factors that might jeopardise benefit realisation • Closer look at outcome data • Qalys/NNTs
There are some common mistakes that need to be avoided when making a business case • Timing is everything • “If you get something at the wrong time you generally put it in the bin” • Budgets and services are parochial • Be careful when trying to sell on a cost saving realised by another department / trust / budget • “Moving funding around is getting better but it is time and energy consuming” • “Projects often founder because there are dependencies or benefits elsewhere in the system” • Using language that is too ‘clinical’ • Information needs to be in a format that more ‘generalist’ purchasers can understand
Good business cases are setting the standard • Business cases need to be comprehensive • Business cases need to be realistic • Anything that enables localities to personalise information is key • “draft protocols that can be amended for local use saves us heaps of time” • Independent review of evidence is persuasive