Download
1 / 15
170 likes | 532 Views
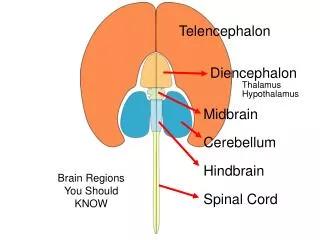
General function Gross features and histology Cerebellar peduncles Cerebellar lobes and functional correlation Cerebellar afferents (input) Cerebellar efferents (output) Clinical Correlation. Cerebellum: Organization and Cerebellar Pathways. I. General function.

E N D
General function Gross features and histology Cerebellar peduncles Cerebellar lobes and functional correlation Cerebellar afferents (input) Cerebellar efferents (output) Clinical Correlation Cerebellum: Organization and Cerebellar Pathways
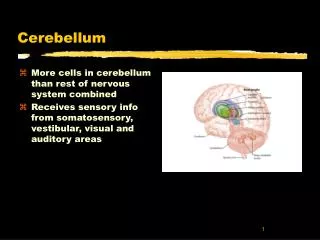
I. General function • Coordinates all movements. • Participates in maintaining equilibrium. • Regulates muscle tone. - In coordinating movements the cerebellum ensures that all muscles contract smoothly. - “synergy” implies that muscles contract in precise spatial and temporal sequences.
II. Gross features and histology (Atlas Figs 82 and 80) Gross • Composed of cerebellar hemispheres and interconnecting vermis. • Longitudinal surface ridges of the hemispheres and vermis are called folium (single), folia (more than one). • White matter (deep and that into the folia) form the arbor vitae (tree of life, seen best in sagittal sections). • Deep cerebellar nuclei (from med to lat) are: fastigial, globose, emboliform and dentate.
II. Gross features and histology (Atlas Figs 82 and 80) Gross • Composed of cerebellar hemispheres and interconnecting vermis. • Longitudinal surface ridges of the hemispheres and vermis are called folium (single), folia (more than one). • White matter (deep and that into the folia) form the arbor vitae (tree of life, seen best in sagittal sections). • Deep cerebellar nuclei (from med to lat) are: fastigial, globose, emboliform and dentate. Histology • Cortex composed of three layers (from pial surface to depth): 1) molecular, 2) Purkinje cell body and 3) granule cell. • Axons of Purkinje cells (cortical output) project to the deep nuclei and mediate GABA inhibition onto deep nuclei cells. • Axons of deep nuclei cells leave the cerebellum (via output fibers) and mediate excitation (glutamate) on motor targets in the brainstem, such as the red nucleus and the ventral lateral nucleus of the thalamus.
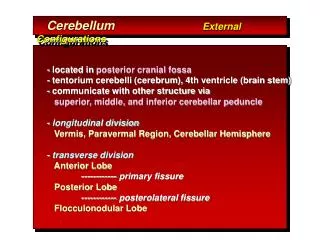
III. Cerebellar peduncles (Atlas Figs 91, 21 and modified 71) • Three white matter peduncles attach the cerebellum to three major divisions of the brainstem: 1) Superior (aka brachium conjuctivum) to midbrain. Composed mainly of efferent fibers from the cerebellum. 2) Middle (aka brachium pontis) to pons. Composed of afferent fibers to cerebellum. 3) Inferior (aka restiform body) to medulla. Composed mainly of afferent fibers to cerebellum. • In addition the juxtarestiform body (seen in Atlas Fig 21) is a thin bundle of fibers sandwiched between the sup and inf peduncles. Interconnects the vestibular cerebellum with the vestibular nuclei.
IV. Cerebellar lobes and functional correlation (Figs 71 and CNS paths XI) • Vermis and hemispheres can be roughly subdivided into three (ant, post and flocculonodular) lobes by primary and posterolateral fissures. However, three longitudinal functional zones are distinguished: 1) Flocculonodular – Part of the vestibulocerebellum (aka archicerebellum). Plays a role in maintaining equilibrium via medialmost axial extensor antigravity muscles. 2) Paravermis of anterior and posterior lobes. Coordinates proximal axial flexor muscle activity through brainstem motor centers. 3) Hemispheres (most of the lat portions of ant and post lobes). Their activities are coordinated with those of the motor cortex. Synergizes skilled movements performed mainly with distal appendicular muscles.
V. Cerebellar afferent (input) fibers (CNS paths X) • DSCT • Conveys unconcious proprioceptive information fromipsilateral trunk and lower limb muscles. • Originates from Clarke’s nucleus (C8-L2 spinal levels). • Axons from Clarke’s nucleus ascend in the ipsilateral DSCT and enter cerebellum with the inf cerebellar peduncle. Axons give off collaterals to globose and emboliform nuclei and terminate in cortex of ant lobe and vermis of post lobe. • Cuneocerebellar tract • Conveys unconscious proprioceptive information from ipsilateral upper limb and neck muscles. • Originates from accessory cuneate nucleus at caudal and midmedulla levels. • Axons pass into the cerebellum with the inf cerebellar peduncle. After giving off collaterals to globose and emboliform nuclei, axons terminate in cortex of ant lobe and vermis of post lobe.
Afferents (cont.) • ASCT • It acts asan internal feedback connection that monitors descending “motor” signals destined to spinal motor neurons. • Originates from ventral horn at lumbosacral spinal levels. • Axons first cross midline in the spinal cord and join the ASCT. Same axons ascend up to the pons where they join the sup cerebellar peduncle to enter the cerebellum. Once in the deep white matter of the cerebellum, the axons recross the midline, give off collaterals to the globose and emboliform nuclei and terminate in in the cortex of ant lobe and vermis of post lobe.
Afferents (cont) 4) Vestibulocerebellar fibers • Direct (vestibular nerve) and indirect (relay in the vestibular nuclei) pass into the cerebellum via the juxtarestiform body. • Fibers terminate in the ipsilateral flocculonodular lobe and uvula after giving off collaterals to the ipsilateral fastigial nucleus • Part of circuits underlying changes in posture and eye movements in response to head movement. 5) Pontocerebellar tract • Part of cortico-ponto-cerebellar circuit (links activity of the cerebral cortex with that of the cerebellum). • Originates in (basilar) pontine nuclei. • Large number of fibers cross the midline of basilar pons and enter the middle cerebellar peduncle. Same fibers give off collaterals to the contralateral dentate nucleus and then terminate throughout the cortex of paravermis and cerebellar hemisphere. • Functions to coordinate mostly voluntary, skilled movements.
Afferents (cont) 6) Olivocerebellar tract • Originates in the inf olivary nucleus. • Cells in the inf olivary nucleus receive both descending and ascending info from motor and sensory centers in cerebral cortex, brainstem (e.g., red nucleus) and spinal cord. • Fibers of the olivocerebellar tract are entirely crossed and enter the contralateral inf cerebellar peduncle. Once in the cerebellum, fibers give off collaterals to globose, emboliform and dentate nuclei and terminate in all cerebellar cortical areas as “climbing” fibers. • Climbing fibers strongly stimulate Purkinje cells in an almost 1:1 relationship. • Function in learning motor skills that require trial and error.
Cerebellar efferent (output) fibers (Atlas CNS paths XI) • Output of cortex (Purkinje cells) is inhibitory (GABA) to deep nuclei. Output of deep nuclei is excitatory (glutamate) to targets in the brainstem (e.g., red nucleus, VL). Three outputs from cerebellum are considered here: • Cerebello-rubro-thalamic. • Originates from globose, emboliform and dentate nuclei. • Axons from those nuclei contribute to most of the sup cerebellar peduncle (SCP) which leaves the cerebellum and ascends to caudal midbrain where it crosses entirely to opposite side. • Fibers of crossed SCP from globose and emboliform ascend to rostral midbrain where they terminate in the red nucleus (RN). Those from dentate continue ascending and terminate mostly in the ventral lateral (VL) nucleus of the thalamus. • VL projects to primary motor cortex (Brodmann’s area 4) where most of the cerebellar correction of skilled (mostly voluntary) and some associated (automatic) movements are carried out. • RN facilitates spinal motor neurons which innervate flexors involved in associated movements. Cerebellar correction by way of SCP occurs here.
Efferent fibers (cont) 2) Cerebello-vestibular fibers. • Each fastigial nucleus projects bilaterally to the vestibular nuclear complex. • Vermis of ant lobe projects to a portion of vestibular nuclei (note that this is the only exception where Purkinje cell axons leave the cerebellum). • Vestibular nuclei send two descending paths (lat and med vestibulospinal tracts) to spinal cord for control of axial extensor antigravity muscles and an ascending path (asc MLF) for eye movement control. • This is how cerebellum controls coordination of muscles while individual maintains equilibrium. 3) Cerebello-reticular fibers. • Are bilateral and diffuse. • Originate from all 4 deep nuclei and terminate in the reticular formation of the pons and medulla. • Generally function to mostly enhance muscle tone.
VII. Clinical correlation • Three major syndromes are distinguished depending which of the functional zones of the cerebellum is compromised: • Archicerebellar syndrome. Usually results from a midline tumor (medulloblastoma), but it can be produced by trauma or disease of the flocculonodular lobe. Signs include trunkal ataxia, inability to maintain upright posture and falling backwards to either side. Rotational nystagmus may also be present. • Paleocerebellar syndrome. Usually results from lesions or atrophy (thiamine defficiency) of the ant lobe. Patients exhibit locomotor ataxia, hypotonia, dysmetria and abnormal heel-to-shin test. • Neocerebellar syndrome (lat zone). Usually from tumors in the lat hemispheres which may impinge on the deep nuclei. Signs and symptoms include: hypotonia, locomotor ataxia, dysmetria, dysdiadochokinesia, decomposition of movements, dysarthria, nystagmus on lateral gaze and intention tremor. Lesions in the SCP bring about most of these signs. However, whether they occur ipsi or contralateral to the lesion depends on the level of the lesion caudal to or rostral to the SCP decussation.