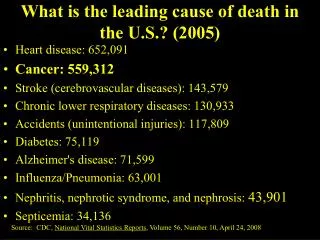
Download
1 / 26
290 likes | 566 Views
CHAPTER 17 Cognitive Impairment, Alzheimer’s Disease, and Dementia. Normal Changes in Cognition. Cognition comprises intelligence, learning, judgment, reasoning, knowledge, understanding and memory. Normal age-related changes in cognition Slower response times Loss of short-term memory

E N D
CHAPTER 17Cognitive Impairment, Alzheimer’s Disease, and Dementia
Normal Changes in Cognition • Cognition comprises intelligence, learning, judgment, reasoning, knowledge, understanding and memory. • Normal age-related changes in cognition • Slower response times • Loss of short-term memory • Confusion not a normal part of aging
The Five “Ds” of Confusion • Delirium– acute onset • Causes • Metabolic disorder • Infections • Fever • Dehydration • Damage – acute onset • Causes • Stroke • Head injury • Exposure to chemicals (Cont’d…)
The Five “Ds” of Confusion (…Cont’d) • Deprivation – variable onset • Causes • Sensory impairment • Social interaction • Depression – subacute onset • Causes • Loss • Metabolic imbalances • Drugs • Inner sadness (Cont’d…)
The Five “Ds” of Confusion (…Cont’d) • Dementia – slow onset • Causes • Cardiovascular disease • Metabolic problems • Alzheimer’s disease • HIV
Delirium • A sudden change of consciousness that occurs rapidly • Signs and symptoms • Disorganized thinking • Decreased attention span • Lowered or fluctuating level of consciousness • Disturbance in sleep-wake cycle • Disorientation • Changes in psychomotor activity • Sometimes, delusions or hallucinations • Usually, agitation and hyperactivity • Sometimes, hypoactive behavior such as lethargy and reduced activity
Finding the Cause • Pain • Constipation • High or low body temp (extreme) • Alcohol use • Lack of oxygen to brain • malnutrition
Treatment • Depends on cause • Treat the source • Supportive Care • Low stimuli environment • Have them wear hearing aids/glasses • Clocks and calendars • Ambulate often if allowed
Dementia • Classified as Alzheimer’s or non-Alzheimer’s • In early stages is difficult to differentiate from age-associated memory impairment • Decreasing ability to process new information and to retrieve and use the information accumulated throughout life
Dementia • Causes- • More than 60 • Metabolic problems • Hormonal • Infections • Brain trauma • Tumors • Pain • Sensory deprivation • Chemical • Anemia • Drug interactions
Dementia • Slow gradual onset • Attempt to hide impairments • Most common early symptom is declining memory
Sundowners • Group of behaviors characterized by confusion, agitation and disruptive actions that occur IN LATE AFTERNOON OR EVENING • Cause is unknown • Associated with dementia, physical or social stressors • Box 16-3
Alzheimer’s Disease • A progressive, degenerative disorder that affects brain cells and results in impaired memory, thinking, and behavior • Cause is unknown • 50% of all cases of dementia have Alzheimer’s Disease. • Some 250,000 new cases per year • Post mortem the brain reveals shrunken and with abnormal tangles of nerve fibers (Cont’d…)
Left- normal Right – Alzheimer’s
Alzheimer’s Disease (…Cont’d) • Signs and symptoms • Memory loss • Difficulty performing familiar tasks • Problems with language • Poor judgment • Problems with abstract thinking • Misplacing things • Disorientation to time and place • Loss of initiative • Changes in mood or behavior • Changes in personality
Stages of Alzheimer’s Disease • Early stage • Begins with the loss of recent memory and progresses to strange behaviors and mood swings • Intermediate stage • Clients cannot recall recent events or process new information and eventually lose all sense of time and place. They are still ambulatory but at high risk for falls and injury. • Severe stage • Clients are unable to do anything and are entirely dependent on others. • End stage • Clients slip into a coma.
Losses of Alzheimer’s • Robbed of “personhood” • Affective loss- drain of one’s personality • Conative loss- inability to carry out plans for the simplest activities • Catastrophic reactions- minor anxiety cascade • Confused • Agitated • fearful
Health Care Goals for Clients with Alzheimer’s Disease • Provide for clients’ safety and well-being • Bathing, grooming, eating, physical activity • Remember that clients have no sense of safety or danger. • Manage clients’ behaviors therapeutically • Gently redirect clients who are behaving inappropriately to less stressful activities. • Music therapy, validation therapy, and exercise help reduce stress. (Cont’d…)
Health Care Goals for Clients with Alzheimer’s Disease (…Cont’d) • Support for family, relatives, and caregivers • Important sources of information about clients • Should be included in planning care for clients • Provide respite care • Informal support groups–family members, friends, and people who knew the family member before AD • Formal support groups • Offered by the Alzheimer’s Association, home care agencies, and elder care centers
Therapeutic Interventions • Provide for safety and well-being • Manage behaviors therapeutically • Proved support for family and caregivers • Gentle redirection • Music therapy, validation, sensory stim
Interventions by stage • Early- • Cholinesterase inhibitors • P 175 top • Cognitive training • Orientation • Monitor personal hygiene • Daily routine • Home eval for safety
Middle/Late Stage Behavior gradually becomes disorganized personal hygiene, eating and elimination neglected Wandering is most serious problem 60% will wander and become lost in commun. Offensive behaviors need to looked at as COMMUNICATION OF UNMET NEED
As late stage progresses • High risk for : malnutrition, pneumonia and pressure related wounds
Caregivers • Support • 70% of alzheimer’s are cared for in the home by family, friends and home care staff • Find a balance between personal needs and those of the loved one • Informal support groups • Formal support groups • Education- • Stress levels decrease with adequate training