Download
1 / 43
460 likes | 1.06k Views
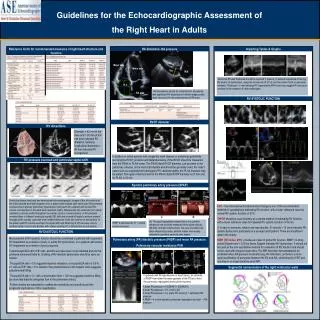
THE ECHOCARDIOGRAPHIC EVALUATION OF THE HEART FAILURE PATIENT. Prof. Patrizio Lancellotti, MD, PhD, University hospital, CHU Sart Tilman, Liège. Potential Role of Echo in Heart failure . Bedside non-invasive imaging tool Low cost and no radiation exposure Goals

E N D
THE ECHOCARDIOGRAPHIC EVALUATION OF THE HEART FAILURE PATIENT Prof. Patrizio Lancellotti, MD, PhD, University hospital, CHU Sart Tilman, Liège
Potential Role of Echo in Heart failure • Bedside non-invasive imaging tool • Low cost and no radiation exposure • Goals • To highlight the underlying cardiac disease • To quantify systolic-diastolic dysfunction and hemodynamics • To match symptoms and cardiac involvement • To stratify the prognosis • To guide the therapy • Potential benefit : “ The importance of being earlier ”
100 90 80 Congestive HF 70 60 Treated but no Congestive HF Echo 50 Event-free survival (%) 40 p<0.01 Congestive HF + Appropriate therapy No-echo 30 20 10 0 0 12 24 36 48 60 72 Time (months) HEART FAILURE THERAPY • Diagnosis of HF • Symptoms : dyspneoa or fatigue (rest or exer) • Objective evidence of cardiac dysfunction (echo) Senni et al., J Am Coll Cardiol 1999,33:164 Guidelines of the ESC 2005
Back to reality ¡¡¡ Euro Heart Failure Use of Echocardiography % Cleland et al Lancet 2002
Establishing the diagnosis of HF • Is LV ejection fraction preserved or reduced ? • Is the LV structure normal or abnormal ? • Other structural abnormalities ?
Establishing the diagnosis of HFSystolic vs diastolic dysfunction Diagnosis of diastolic HF (up to 40%) Abnormal LV EF < 50%
Establishing the diagnosis of HFSystolic vs diastolic dysfunction • Modified Simpson’s Method of discs • Endocardial Border ? • Load dependent • Geometric assumptions • Foreshortening in 90% • Accuracy ? 4C 2C
Establishing the diagnosis of HFDiastolic Heart failure • Symptoms or signs of HF • Normal or midly abnormal LV EF (≥ 50%) (LV EDVI < 97 ml/m², LVESV < 49 ml/m²) • Evidence of abnormal LV relaxation/distensibility
Does “pure” diastolic dysfunction exists ? Sv LV velocities (Sv) Radial function DHF Sv < 6.5 cm/s Longitudinal function EF < 45 % SHF “Natural”evolution of heart failure
Diastolic function + LV filling pressure E Vp A Nl > 55 cm/s E’ Nle > 8 cm/s
E/E’ > 15 EF > 50%+ EDVI < 97 ml/m² 15 > E/E’ > 8 NTproBNP > 220 Or BNP > 200 Echo-Doppler Ap-Am > 30 ms or LAVI > 40 ml/m² or LVMI > 122 (149) g/m² or Atrial fibrillation Heart failure with normal ejection fraction Evidence of diastolic dysfunction ? (E/A ? related to age) Paulus W et al, Eur Heart J 2007; epub
Evidence of diastolic dysfunction ? E/E’ > 15 EF > 50%+ EDVI < 97 ml/m² NTproBNP > 220 or BNP > 200 Echo-Doppler Ap-Am > 30 ms or LAVI > 40 ml/m² or LVMI > 122 (149) g/m² or Atrial fibrillation E/E’ > 8 Heart failure with normal ejection fraction Paulus W et al, Eur Heart J 2007; epub
Diastolic stress echocardiography LVEDP elevated only during exercise in 24% REST EXER Supine bicycle ergometry during cardiac catheterisation in 37 patients, mean EF 58% Septal annulus E/E’ increased 12.1 to 17.1 E/E’ > 13 at exer 90% specificity of reduced exercise capacity Mean 18.0 Mean 13.2 REST EXER E/E’ 8 E/E’ 16 Burgess MI et al, J Am Coll Cardiol 2006; 47: 1891-900
Ultrasound lung comets ULC are a simple echographic sign of increased extravascular lung water due to thickening of interlobular septa Lichtenstein D et al. Intensive Care Med 1998;24:1331-1334 Jambrik Z, Picano E et al. Am J Cardiol 2004;93:1265-1270
Stress comet The variation between postexercise and baseline ULC score correlated significantly with: • the variation between peak stress and rest PCWP (r = 0.62, p =.0001) • systolic pulmonary artery pressure (r = 0.44, P = .0001) • wall-motion score index (r = 0.30, P = .01) • peak stress E/Em (r = 0.71, P = .0001) ULC is a sensitive and accurate marker able to detect pulmonary interstitial edema even before it becomes apparent clinically Agricola E, Picano E et al. J Am Soc Echocardiogr 2006
PULMONARY PRESSURE PASP RAP PASP = 4 V² max + RAP Nl 2 – 2.5 cm/s • Underestimation of pressure if inadequate envelope • Enhanced signal by injecting agitated saline solution D exp – D insp D exp VC diameter IVC changes RAP < 1.5 cm collapsus 0-5 1.5-2.5 cm > 50% 5-10 > 2.5 cm < 50% 10-15 > 2.5+HV dilation No change > 20 Simplified Bernoulli equation : not applicable
RV FUNCTION RV FUNCTION TAPSE • EF Load dependency • TAPSE : (Nl > 24 mm) • * if < 8.5 mm, RV EF < 25% • * < 14 mm bad prognosis • TDI Tricuspid systolic annulus vel : • * if < 11.5 cm/s, RV EF < 45% • IVA < 2.52 m/s², RV dP/dt, …. • Meluzin JASE 2005;18:435 TASv IVA * Less accurate in severe TR Hsiao S JASE 2006;19:902
MANAGEMENT OUTLINE • ESTABLISH HEART FAILURE • DISTINGUISH SYSTOLIC VS DIASTOLIC DYSFUNCTION • DETERMINE AETIOLOGY • IDENTIFY POTENTIALLY CORRIGIBLE LESIONS • ASSESS PROGNOSIS • CHOOSE APPROPRIATE MANAGEMENT
CAUSES OF HF ACC/AHA 2005 Guidelines for CHF Heart failure Reviews,2003
DEGENERATIVEMyxomatous : flail leaflet Failure of valve tip coaptation
MANAGEMENT OUTLINE • ESTABLISH HEART FAILURE • DISTINGUISH SYSTOLIC VS DIASTOLIC DYSFUNCTION • DETERMINE AETIOLOGY • IDENTIFY POTENTIALLY CORRIGIBLE LESIONS • ASSESS PROGNOSIS • CHOOSE APPROPRIATE MANAGEMENT
Prognostic indicators Abnormality Mild Moderate Severe LV ESV (ml/m²) <30 30-60 >60 LV EF (%) 45-54 44-30 <30 Peak Sv (cm/s) < 6 4-6 ≤ 3 E/A Gr I Gr II-III Gr IV Mitral DT -- -- <130 E/Ea <8 8-15 >15 Ea (cm/s) -- -- <3 Lung comets 5-15 16-36 >30 MR (ERO:mm²) <10 10-20 >20 LV dP/dt (mmHg/s) 550 450-450 <450 LA volume (ml/m²) -- -- >68 WMSI 1-1.5 1.5-1.8 >1.8 RV dysfunction -- -- +
100 Patients with out intra-LV asynchrony 90 80 70 60 Event-free survival (%) 50 40 p<0.001 Patients with intra-LV asynchrony 30 20 10 0 0 50 100 150 200 250 300 350 Days New Prognostic indicators : Dyssynchrony 86 ms 132 ms Ao Pulm Interventricular asycnhrony Care HF. Eur H J 2007 Bader et al. J Am Coll Cardiol 2004;43:248
« No single measure of mechanical dyssynchrony may be recommended to improve pt selection for CRT » High Echo lab variability Need for standardization
Criteria for the selection Major ?Intraventricular asynchrony - LV dispersion 65 ms - TPS SD 12 31 ms Others ? Inter + Intra V delay > 102 ms Septal-to-posterior delay > 130 ms Interventricular delay > 40 ms Aortic pre-ejection time > 140 ms LV filling time < 40 % of cardiac cycle Diastolic mitral regurgitation SD 16s 3D > 8.3%
Prognostic indicators : ischemic MR MI > 6 months No NYHA IV MI > 16 days NYHA Class IV Grigioni et al Circulation 2001, 103; 1759 Lancellotti et al Circulation 2003, 108:1713
Prognostic indicators : ischemic MR MI > 6 months No NYHA IV MI > 16 days NYHA Class IV Grigioni et al Circulation 2001, 103; 1759 Lancellotti et al Circulation 2003, 108:1713
STRESS ECHO dynamic MR Lancellotti et al Circulation 2003, 108:1713 Lancellotti et al, Eur Heart J 2005, 26:1528 Peteiro et al, Eur J Echo 2007 Piérard et Lancellotti. N Engl J Med 2004,351:1627
STRESS ECHO in Aortic Stenosis with low gradient Operative mortality 5% ( 3 of 64 pts) if CR + 32% (10 of 35 pts) if CR- Low-gradient AS mean gradient < 25 - 30 mm Hg calculated AVA < 1.0 cm² Dobutamine-responsiveness : (class IIa) Contractile reserve SV ≥ 20% Monin et al , Circ 2003
30 25 20 15 10 5 0 STRESS ECHO : Viability and Ischemia Sustained improvement -79.6% χ2=147 p<0.0001 23% χ2=1.43 p<0.23 Ischemic 16 Mortality (%) 7.7 6.2 3.2 RVS (n=728) MED (n=483) RVS (n=366) MED (n=579) VIABLE NO VIABLE Picano Circulation 1998 Allman et al. JACC 2002;39:1151 Pratali L et al,Am J Cardiol 2001
MANAGEMENT OUTLINE • ESTABLISH HEART FAILURE • DISTINGUISH SYSTOLIC VS DIASTOLIC DYSFUNCTION • DETERMINE AETIOLOGY • IDENTIFY POTENTIALLY CORRIGIBLE LESIONS • ASSESS PROGNOSIS • CHOOSE APPROPRIATE MANAGEMENT
TREATMENT OF HEART FAILURE Medications (Acute; Chronic: LV remodeling; Hypotension) Heart transplantation Revascularisation of hibernating myocardium Mitral valve repair Resynchronisation therapy (CRT)
Adaptation of Loop DiureticsReversibility under treatment and prognosis Survival free of transplantation • Group 1A: n=24 • Irreversible restrictive profile • Group 1B: n=29 • Reversible restrictive profile • Group 2: n=57 • Non restrictive profile Pinamonti B et al, JACC 1997;29(3):604
Adaptation of Beta Blockers Clinical trials: 12% Beta-blockers are not tolerated Capomolla et al. JACC 2001;38:1675-84
LV REVERSE REMODELING Effects of treatment Criteria of reverse LV remodeling (EDD, FS et LV mass) ESV 10-15% Survival Cv events Kawai et al, Am J Cardiol. 1999 Sep 15;84(6):671-6
Stress echo : LV Viability/Ischemia EF < 35% No or limited Viability Viability > 4 segments Medical therapy Revascularization Resynchronization Good responder Bad responder Transplantation Allman et al. JACC 2002;39:1151
HOW TO CORRECT FUNCTIONAL MR ? TTE pre-op - Coaptation height ≥ 1 cm - Tenting > 2.5-3 cm² - PLA > 45 °, lateral WMA - Central jet or Complex jets - EDD > 65 mm, ESD > 51 mm Braun EJCS 2005; Shiota AJC 2006,98; Calafiore ATS 2004, 77; Magne Circ 2007,115;782-791
CRT OFF CRT ON
Echo in Heart Failure Structural abnormalities LV function Lung comets EF, Volumes, TDI Sv, E/Ea MR Stress echo Evaluation of risk Treatment No one single echo parameter represents a magic number Choose clinical strategy only after obtaining confirmation from several matching parameters