Download
1 / 42
420 likes | 733 Views
Micro-cost Methods of Finding VA Costs Mark W. Smith, PhD Paul G. Barnett, PhD HERC Economics Course March 16, 2005 Methods described in this talk Direct measurement Pseudo-bill Reduced list costing Clinical cost function Estimate Medicare inpatient payment

E N D
Micro-cost Methods of Finding VA Costs Mark W. Smith, PhD Paul G. Barnett, PhD HERC Economics Course March 16, 2005
Methods described in this talk • Direct measurement • Pseudo-bill • Reduced list costing • Clinical cost function • Estimate Medicare inpatient payment
Method # 1: Direct Measurement • Used to the find the cost of: • innovative care • care unique to VA • Method • Measure staff activity • Find labor cost • Find cost of supplies, capital, overhead
Staff activity analysis • Methods of finding staff activities • Time and motion study • Individual staff keeps log of own activity • Individual estimates own activities • Supervisor estimates staff activities • Need not be comprehensive; can sample activity
Characterizing Staff Activities • Cost of patient care may include non-patient care time • Activities that produce several products may need to be included, depending on perspective • e.g., time spent on clinical research may be regarded as a research cost, or a patient care cost, depending on analytical goal
Staff Activity Analysis for Treatment Innovations • Should not include development cost • Should measure when program fully implemented, e.g., with typical productivity
Other costs • Survey or actual measure of supply costs • Alternatives for overhead • Cost report data • Standard rates • Alternatives for capital • Cost report • Rental rates
Finding VA labor cost Data Sources: • VA Payroll System: PAID • VA General Ledger: Financial Management System (FMS) • DSS ALBCC reports
PAID • VA Payroll data • Detailed to the individual • Confidential, requires special permission to gain access • Useful when FMS and DSS have insufficient detail
Financial Management System (FMS) FMS reports cost and hours • By Station (medical center) • By Sub-Account • Approximately 72 personnel types • 1081 Physicians, full-time • 1061 Registered nurses • Contract expenses, supplies, etc.
DSS ALBCC ALBCC = Account Level Budgeter Cost Center • Draws from FMS and DSS data. Unlike FMS, includes contract labor expenses • Same sub-accounts as FMS • Estimated wages are typically slightly less in ALBCC than in FMS
Finding Average Compensation • FMS & DSS report all labor costs, incl. benefits and employer contributions to taxes • We used the end-of-fiscal-year report (Sept.) to find average employee salaries • Both DSS and FMS for comparison
Recommendations • Caution! Do not double count payroll! Use either payroll analysis (BOC 1000-1099) or personnel services (BOC 1100-1199). • Activity surveys should use job categories found in VA data.
Resources Full FMS & DSS data at AAC. Summary data in KLFMenu. More on FMS in Volume IV of the “Blue Books” and HERC Technical Report #12 (Smith & Velez 2003) on the HERC web site: www.herc.research.med.va.gov/pubs.htm
Finding unit cost with direct measurement • Average cost • Total program cost/number of units • Assumes homogeneous products • Relative Values needed for heterogeneous products • Find Relative Value of each product • Find cost per relative value unit (RVU) • Use this to find cost of each product
Method # 2: Pseudo-bill • Itemize all services utilized • Use schedule of cost/reimbursement for each service
Method # 3: Reduced list cost • Some utilization items in pseudo-bill explain most of variation in cost • E.g., laboratory tests correlate with number of surgical procedures • Reduce list of utilization items may be sufficient • Schedule of cost/reimbursement must be adjusted • E.g., new rate for surgical procedures, including cost of laboratory
Method # 4: Cost Function • Useful for estimating inpatient cost • Function is used to simulate costs • Estimated from external data on cost and characteristics of stays (not from own study data) • Obtain characteristics of stay from own study • Apply function to estimate cost of stay • Advantage: fewer variables than a pseudo-bill Disadvantage: could have large error for individual bills
Cost function • Dependent variable is cost-adjusted charge from non-VA data • Typical independent variables: • Diagnosis Related Group (or HCCs, ADGs, etc.) • Diagnoses (1 or more binary vars.) • Procedures (1 or more binary vars.) • Vital status at discharge • Length of stay • Days of ICU care
Transformation of Dependent Variable • Cost data skewed • Skewness violates assumptions of ordinary least squares (OLS) • Error terms not normally distributed with identical means and variance • Transformation • Typical method: log of cost • can make OLS assumptions more tenable
Correcting Re-transformation Bias • Model of form • Cannot simulate cost for X=XO by taking exponent of fitted regression
Retransformation bias • The expected value of cost is:
Smearing estimator for log transformed regression • The right term is the smearing estimator = the mean of the anti-log of the residuals • See: Duan, N. (1983) Smearing estimate: a nonparametric retransformation method, Journal of the American Statistical Association, 78, 605-610.
References for Retransformation • Manning WG, Mullahy J. Estimating log models: to transform or not to transform? J Health Econ 2001 Jul;20(4):461-94. • Basu A, Manning WG, Mullahy J. Comparing alternative models: log vs Cox proportional hazard? Health Economics 2004 Aug;13(8):749-65. • See HERC web site FAQ response: www.herc.research.med.va.gov/faqE2_retransformation.pdf
Method # 5: Estimating Medicare inpatient reimbursements • Part A -- Prospective Payment for Inpatient Stays • Part B -- Payment for Physician Services to Inpatients
Medicare Facility Payment: Inpatient • Standard payment for DRG of the stay, adjusted by • Disproportionate Share Provider payments • Medical education • Capital • Outlier • Geographic adjustments • Medicare pays flat rate per DRG, regardless of length of stay • Cost analysis may wish to capture effect of length of stay on cost
Prospective Payment System PC Pricer • Computer application for calculating facility payment • Requires • 6-digit hospital PPS (identifier) - DRG • Admission and discharge dates (= LOS) • Optional: cost outlier, patient transferred • Incorporates adjustments for geography, teaching, disp. share, etc. • New version each year • Limitations • Excludes physician payment • Payment economic cost Pricer: www.cms.hhs.gov/providers/pricer/pricdnld.asp#inp Provider IDs: www.cms.hhs.gov/providers/hipps/ippspufs.asp#psf
Medicare Facility Payment: Outpatient • Payment based on CPT procedure codes • Most CPTs assigned an Ambulatory Payment Classification (APC) group with an associated cost • Some CPTs have no APC: • Paid on cost pass-through basis • Paid through another APC (e.g., anesthesia) • Paid through a separate cost list • Multiple CPTs assigned to a single group-APC • Some surgery procedures are discounted • See documentation for HERC Outpatient Average Cost data: www.herc.research.med.va.gov/Pubs.htm
Medicare Provider Payment: Outpatient • Medicare distinguishes (inpatient) facility-based providers from (outpatient) office-based providers • We assume that all VA care is facility-based • Sum of inpatient facility and provider payments typically exceeds single outpatient payment
Estimate Inpatient Physician Payment • Urban Institute determined average Part B physician payment • Reported as RVU weights for each DRG • Miller, M. E., & Welch, W. P. (1993). Analysis of Hospital Medical Staff Volume Performance Standards: Technical Report (6210-01). Washington D.C.: The Urban Institute
Which method should I use? • Direct measurement • Pseudo-bill • Reduced list costing • Clinical cost-function • Estimate Medicare inpatient payment Barnett PG. Determination of VA health care costs. Medical Care Research and Review 2003;60(3 Suppl.):124S-141S.
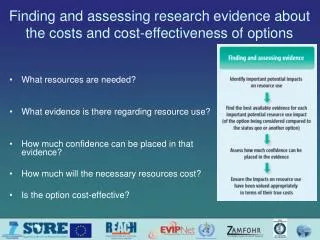
Criteria for selecting a micro-cost method • Data available? [consent, cost to obtain] • Method feasible? [time, cost, data granularity] • Assumptions appropriate? • Method accurate? • Will it capture the effect of the intervention on resource use?
Method #1: Direct Measurement • Assumptions • Activity survey and payroll data are representative • May assume all utilization uses the same amount of resources • Advantages • Useful to determine cost of a program that is unique to VA • Disadvantages • Limited to small number of programs • Can’t find indirect costs • Can’t find total health care cost
Method #2: pseudo-bill • Assumptions • Schedule of charges reflects relative resource use • Cost-adjusted charges reflect VA costs • Advantages • Captures effect of intervention on pattern of care within an encounter • Disadvantages • Expense of obtaining detailed utilization data
Method #3: Reduced List Costing • Assumptions • Items on reduced list are sufficient to capture variation in resource use • Cost of items on reduced list is accurate • Advantages • Requires less data than pseudo-bill • Disadvantages • Needs to find data on cost associated with items on reduced list
Method #4: Cost Function • Assumptions • Cost-adjusted charges accurately reflect resource use • The relation between cost and utilization is the same in the current study as in the previous study • Advantages • Less effort to obtain reduced list of utilization measures than to prepare pseudo-bill • Disadvantages • Must have detailed data • Data from prior study may have error or bias
Method #5: Estimate Medicare payment • Assumptions • Medicare payment reflect economic cost • Inpatient: DRG captures effect of intervention on resources used • Advantage: easy to implement • Disadvantages: • Accuracy limited – VA may have different cost structures from average non-VA facilities • Inpatient: doesn’t reflect variation in resources beyond DRG (or LOS)
Combining Methods • No single method may fill all needs, even within a single study • Hybrid method may be best • Direct method or pseudo-bill on utilization most affected by intervention • Cost function or Medicare payment for other utilization
Resources Medical Care Research and Review 2003 (vol. 60, no. 3 Suppl.) - Direct measurement - Pharmacy data - Choosing a method Supplement available from HERC by request HERC web site: FAQ responses, technical reports HERC Help Desk (herc@med.va.gov)
Resources Articles on estimating the private-sector cost of services provided by VA: - acute inpatient - outpatient services - specialized inpatient - VA providers - nursing home care - assistive devices Medical Care 2003 (vol. 41, no. 6 Suppl.)