Download
1 / 27
280 likes | 742 Views
PEDIATRIC HEAD AND NECK MASSES: INTERVENTIONAL RADIOLOGICAL MANAGEMENT . WILLIAM E. SHIELS II , D.O. Chairman Children’s Radiological Institute and Department of Radiology Children’s Hospital Columbus, Ohio. GOALS Provide imaging management update Diagnostic imaging approach

E N D
PEDIATRICHEAD AND NECKMASSES:INTERVENTIONALRADIOLOGICALMANAGEMENT
WILLIAM E. SHIELS II , D.O.ChairmanChildren’s Radiological Institute andDepartment of RadiologyChildren’s HospitalColumbus, Ohio
GOALS Provide imaging management update Diagnostic imaging approach Current state of the art Interventional Radiology Dx role Therapeutic options Pediatric Head and Neck
FOCUS Congenital Inflammatory Neoplastic Benign Malignant PediatricHead and Neck
Highly vascular tumor-benign Male predilection, 7-21 yrs Often present with epistaxis Nasopharynx, max/sphenoid sinuses CT +Contrast for Diagnosis Embolization prior to surgery Juvenile Nasal Angiofibroma
Non-suppurative Sonography for diagnosis Suppurative- neck abscess US guided drainage US guided Bx, FNA Esp. cat scratch, mycobacterial Cervical Adenitis
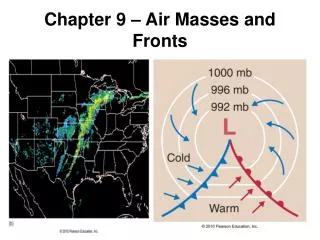
Not acute emergency May compromise airway Bacterial: Grp A. Strep; Staph CT best to diagnose, Sono to Tx Dissects laterally, up, down May dissect to mediastinum extrapleural Complicated Neck Abscess
Branchial cleft remnants Second BC most common Cysts, sinuses, fistulae Same course to tonsillar fossae Unilocular cyst, +/- infection US or CT/MR for diagnosis Successful percutaneous ablation Branchial Cleft Cyst
Venous and lymphatic malformations Slow flow MRI and US (pre-treatment) Arteriovenous malformations High flow, no ST mass MRI, angiography (pre-treatment) Vascular Malformations
Lymphatic ductal malformation Posterior triangle most common Any space in neck, shoulder, Mediastinum, may invade airway Macrocystic (hygroma), microcystic Non-operative treatment +/- successful Lymphatic Malformation
Dual-DrugTime Limited ContactSclerotherapy of Cervicofacial Lymphatic Malformations
DETERGENT (Sotradecol) Opens cellular channels Lipoprotein membrane ETHANOL Denatures proteins Cell destruction Inflammatory response MECHANISM
LOCATIONS Neck Face (including parotid bed) Orbit (retrobulbar) - TYPES Macrocystic Microcystic LOCATIONS / TYPES
US guided puncture 5 F Pigtail Complete aspiration
•Cystic mass-salivary glands Sublingual, submandibular, parotid Dilated ducts…to…..massive cysts Intraparenchymal cystic collections Huge “diving” ranulas in neck spaces RANULA
Pseudocyst Sublingual, submandibular most common Treat infection Drain cystic collection: Mucous Sclerose cavity Regional ablation of salivary gland PLUNGING RANULA
•Cystic mass-salivary glands Sublingual, submandibular, parotid Dilated ducts…to…..large cysts Intraparenchymal cystic collections Usually rupture into mouth, decompress Tx: Percutaneous ablation first line therapy Surgical resection if ablation fails SIMPLE RANULA
Cystic mass-head and neck Developmental origin Lines of embryonic suture closure Periorbital, anterior neck, nose, scalp Lined-keratinizing squamous epithelium Contain epithelium, sebum, debris Percutaneous ablation now an option EPIDERMOID/DERMOID
13 mo male H/o fall from Powerwheel Face first, left eye trauma Periorbital cellulitis T= 103oF CASE HX
CONCLUSION Brief summary- common concerns Pathologic understanding Practical issues Imaging management rationale Therapeutic intervention options Pediatric Head and Neck Masses