Download
1 / 18
180 likes | 359 Views
Atlantic Cardiovascular Patient Outcomes Research Team. CPORT- E Trial Randomized trial comparing outcomes of non-primary PCI at hospitals with and without on-site cardiac surgery. Motivation for Trial. Sustain primary PCI program at no-SOS hospitals Improve access to PCI services

E N D
Atlantic Cardiovascular Patient Outcomes Research Team CPORT- E Trial Randomized trial comparing outcomes of non-primary PCI at hospitals with and without on-site cardiac surgery
Motivation for Trial • Sustain primary PCI program at no-SOS hospitals • Improve access to PCI services • Reduce pressure to create additional cardiac surgery programs • Need for research to inform healthcare policy decisions by state and national organizations
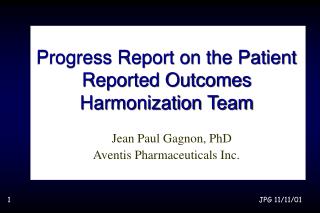
C-PORT Elective NoConsent Registry Not Approached Patient for Diagnostic Cath Refuse Informed consent Consent Registry Catheterization Exclusion criteria Meets inclusion criteria 3:1 Randomization PCI with SOS PCI no SOS
Study Endpoints • Non-inferiority trial • Primary Endpoints • All-cause mortality at 6 weeks • MACE at 9 months • All-cause mortality • Q-wave myocardial infarction • Target vessel revascularization • Assuming 6 week mortality to be 0.8%, a sample size of 18360 was selected to define a non-inferiority margin of 0.4% with a one-sided test for non-inferiority using α=0.05 and β=0.80 for both primary endpoints.
Inclusion and Exclusion Criteria Devices Patient Institution Inclusion • Age > 18 years • Informed consent • > 50% stenosis • All target lesions approachable at no-SOS hospital Exclusion • Unprotected LM • EF < 20% • MD-judged high risk Inclusion • Balloon, stent • Distal protection • Covered stent • Cutting balloon - in-stent restenosis Exclusion • Atherectomy • Cutting balloon- de novo lesion Inclusion • > 200 PCI/year • 24/7 Primary PCI • Complete formal development program • Interventionalist meets AHA/ACC competency
Participating Centers 60 Centers Center Annual PCI Procedure Volume 150 (99,216)median (25th,75th percentile) Median Participation Duration 2.2 years
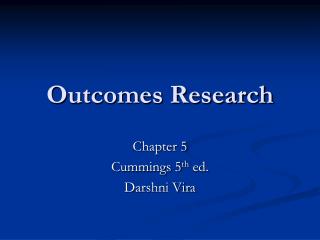
99479 Visits 23805 No Consent 75674 Consented 18867 PCI Randomized 56807 Not Randomized 2298 PCI Excluded (12%)
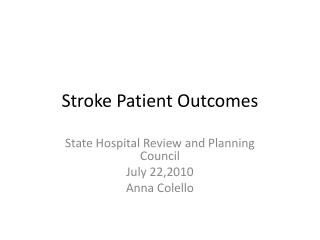
18867 PCI Randomized PCI 18568 (98.4% No PCI 299 (1.6%) Assigned 18496 Unassigned 72 SOS 0.73% No-SOS 0.28% No-SOS 13981 SOS 4515
Presentation Clinical Characteristics Procedure Status * P < 0.001
Baseline Diagnostic Catheterization Totals add up to >100% because Left Main and Graft disease are in addition to disease in the three major circulations
Procedure Characteristics Staged Index PCI procedure requires one or more catheterization laboratory visit dates in addition to the diagnostic catheterization date
PCI Success Patient Success P=0.0096 Lesion Success P=0.0474 PCI Success: <20% residual stenosis and TIMI 3 flow
Mortality 6- Weeks The difference in 6 week mortality is -0.014% with a 90% confidence interval of -0.26% to 0.28%. The upper bound is <0.4%, so that the hypothesis of inferior 6 week mortality for the no-SOS hospitals is rejected at the one-sided P<0.05 level.
Summary • Angiographic Outcomes • PCI Success > 90% in both groups but lower in hospitals without surgery on-site (success rate difference of 1.1% on per patient basis; 0.7% on per lesion basis) • Number of catheterization laboratory visits required to complete the index PCI is greater in patients randomized to hospitals with surgery on-site (1.3 versus 1.7 visits/patient) • Unplanned procedure outcomes • Unplanned catheterization and PCI procedures were uncommon but occurred more frequently in patients randomized to hospitals without surgery on-site (4.4% no-SOS vs 3.4% SOS) • Emergency coronary CABG was rarely required, but was utilized more among patients at hospitals with surgery on-site(0.1% no-SOS vs 0.2% SOS) • Patient Outcomes • Mortality is similar in both groups(0.91% no-SOS vs 0.93% SOS) • The incidence of bleeding, vascular repair, stroke and renal failure is similar in both groups
Conclusion • In hospitals without on-site cardiac surgery that complete a formal PCI development program, adhere to C-PORT participation requirements, and whose outcomes are monitored, non-primary PCI is safe and associated with similar rates of adverse events including mortality. • Long-term, quality outcome data are currently being collected on these study subjects and will be reported early in 2012.