Download
1 / 59
600 likes | 651 Views
Explore the most common malignant disorders of the ovaries, including risk factors, genetic predispositions, and detailed insights into histopathological characteristics of various ovarian neoplasms. Discover the impact of germ cell neoplasms and tumor markers on cancer diagnosis and treatment.

E N D
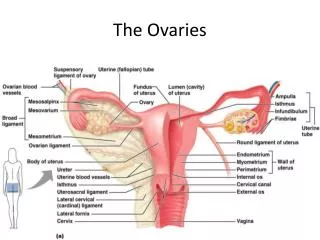
MALIGNANT DISORDERS OF THE OVARIES Assoc. Prof. Gazi YILDIRIM, M.D. Yeditepe University, Medical Faculty Dept of Ob&Gyn
The 5. most common cancer in women • The 5. most frequent cause of cancer death • Lifetime risk 1/70
5-year survival rate • <35% • Mortality has • decreased only • slightly in 30 years • Most diagnosis • made at advanced • disease
RISK FACTORS • Cause of Ovarian Cancer is unknown Risk Factors • High socio-economicstatus • Early menarche • Late menopause • Few children • Never used oralcontraceptive • Genetic (10%) • Environment??? • Dietary factors • Exposure to talc • Exposure to asbestos >90% of ovarian cancer develops sporadically. ~10% of epithelial ovarian cancers are based on genetic predisposition.
GENETIC PREDISPOSITION • Chromosomal abnormalities • Turner syndrome Dysgerminoma, gonadoblastoma • Hereditary ovarian cancer • BOC (breast and ovarian cancer syndrome) • BRCA-1 mutations on chromosome 17 and less commonly BRCA-2 mutations on chromosome 13. • Lynch II syndrome (HNPCC syndrome) • DNA mismatch repair gene mutations • Colon ca, ovarian-endometrial-breast cancer • Acquired genetic abnormalities • P53 tumor supressor gene mutations, HER2/neu proto-oncogene activation
Genetic Predisposition: 5-10% 0f Ovarian Cancer • Carriers of BRCA1 orBRCA2: • 40% risk of ovariancancer • BRCA1 and 2 Germ linemutations: • 10% of all ovariancancers • 1-2% of all breastcancers
HISTOPATHOLOGY OF OVARIAN CANCER 5% of ovarian cancer arises from metastases!! (breast, colon, stomach, endometrium, lymphoma)
EPITHELIAL NEOPLASMS • Derived from the ovarian surface mesothelial cells. • Serous • Mucinous • Endometrioid • Clear cell • Transitional cell • Undifferentiated • Account >60% of all ovarian neoplasms and >90% of malignant ovarian tumors.
Serous Neoplasms • Most common malignant tumor of the ovary. • 35-50% of all epithelial tumors. • Bilateral in 40-60 of cases. • Extraovarian spread at the time of diagnosis in 85% of cases. • Cut section: solid areas,areas of hemorrhage,necrosis, cyst wall invasion and adhesions to adjacent structures.
Histology- serous carcinoma • Mild to moderate nuclear atypia • Psammoma body (irregular calcifications) • The grade of differentiation is based on the degree of preservation of the papillary architecture.
Mucinous Neoplasms • Account for 10-20% of all epithelial ovarian neoplasms • The second most common type of epithelial ovarian cancer. • Bilateral in <10% of cases (in contrast to serous tumors!!!!)
Large size (~16 cm) • Cut sections: multilocular cysts filled with viscous mucin.
Histology- mucinous carcinoma • Composed predominantly of intestinal-like cells that invade surrounding stroma. • Invasive tumors exhibit marked histologic variability from area to area within the tumor. • The differentiation is based on the preservation of the glandlike architecture of the tumor. Extensive sampling required !!
Pseudomyxoma peritonei • Resulting from the progressive accumulation of mucin in the abdominal cavity. • Most commonly in association with low malignant potential. • Also with cystadenocarcinoma of the ovary and appendix, mucocele of the appendix. *potentially morbid secondary to repeated bowel obstruction.
Endometrioid Neoplasm • Exhibits an adenomatoid pattern that resembles endometrial adenocarcinoma. • Bilateral in 30-50% of cases. • Arises rarely in foci of endometriosis (<10% of cases). • The degree of differentiation is based on the extent to which the glandular architecture is retained. • In 30% of cases, there is a synchronous endometrial carcinoma of the uterus A second primary rather than a metastatic focus !!!
Clear Cell Carcinoma • Also referred to as mesonephroid carcinoma • Biologically aggressivehypercalcemia and hyperpyrexia • Difficult to differentiate from mucinous neoplasms the periodic acid-Schiff reaction only weakly (+) in clear cell carcinoma; strikingly (+) in mucinous tumors.
Transitional Cell (Brenner) Carcinoma • Composed of cells that resemble low-grade transitional cell carcinoma of the urinary bladder. • Typically diagnosed at advanced stage disease • Poorer prognosis when compared with that of other histologic types of epithelial ovarian cancer.
Undifferentiated Carcinoma • <10% of epithelial neoplasms. • Characterized by the absence of any distinguishing microscopic features that permit its placement in one of the other histologic categories.
GERM CELL NEOPLASMS • Arise from the germ cell elements of the ovary. • Dysgerminoma • Endodermal sinus tumor • Embryonal cell carcinoma • Choriocarcinoma • Teratoma • Polyembryoma • Mixed germ cell tumors • Occur during the second and third decades of life. • Produce biologic markers which can be monitored to assess response to therapy.
Tumor Markers that may be elevated in the presence of Germ Cell Neoplasms
Dysgerminoma • The female counterpart of the seminoma in the male. • Young females • 30-40% of germ cell tumors. • Unilateral in 85-90% of cases.
Endodermal Sinus Tumor • Second most common germ cell tumor (20%). • Bilateral in <5% of cases. • The most rapidly growing neoplasm !! • Commonly present with an acute abdomen. • Pathognomic finding: Schiller-Duval body • AFP(+)
Immature Teratoma • The malignant counterpart of the mature cystic teratoma or dermoid. • 20% of germ cell tumors. • Bilateral in <5% of cases, although the contralateral ovary commonly contains a dermoid cyst • Immature elements: commonly neuroectodermal
Mature Teratoma (Dermoid) • Common • 20-30 years • The most common tumor diagnosed during pregnancy. • Rarely, the squamous component undergoes malignant transformation over the age 40. (<2%)
Embryonal Carcinoma • Younger patients (mean age of 14 years) • Epithelial cells resembling those of the embryonic disc. • Typically produce hCG • 75% also secrete AFP.
Choriocarcinoma • Primary ovarian choriocarcinoma arises from a germ cell similar in appearance to gestational choriocarcinoma. Nongestational tumors: poorer prognosis * The detection of other germ cell components indicates nongestational tumors!
Gonadoblastoma • Rare tumor composed of nests of germ cells and sex cord derivatives. • More common in the right ovary. • Usually during the second decade of life. • Found in patients with abnormal gonadal development in the presence of a Y chromosome.
Mixed Germ Cell Tumors • 10% of germ cell neoplasms. • Contain ≥2 germ cell elements. • Dysgerminoma and endodermal sinus tumor occur together most frequently.
SEX CORD-STROMAL TUMORS • Heterogeneus group of rare neoplasms originating from the ovarian matrix. cells within matrix have potential for hormon production. Signs and symptoms of estrogen or androgen excess.
Granulosa Cell Tumors • 1-2% of all ovarian tumors. • The most common malignant tumors of the sex cord-stromal tumors. • Hyperestrogenism • Call-exner bodies Precocious puberty in young girls Endometrial hyperplasia and vaginal bleeding in postmenopausal women
Thecoma • Benign • Hyperestrogenism • Lipid-laden stromal cells • Typically develop in postmenopausal women in their mid-60s. Yellow color on cut section
Fibroma • Benign • Meigs’ Syndrome • Ovarian fibroma • Ascites • Pleural effusion • Hormonally inactive Mimic the presentation of ovarian cancer.
Sertoli-Leydig Cell Tumors • Rare • Consist of testicular structures at different stages of development. • Usually virilizing • During the third decade of life • Rarely bilateral
Tumors metastatic to the ovary • 25% of all ovarian malignancies. • Clinically mimic the primary ovarian cancer • Usually present as bilateral adnexal masses • 25% of cases unilateral • Most common primary cancers: breast, stomach, colon and endometrium.
SYMPTOMS • Vague and non-specific !! • Abdominal bloating • Indigestion, dyspepsia • Altered bowel habits • Menstruel abnormalities • Pelvic fullness • Pain
The prepubertal child and the postmenopausal woman are at greatest risk for developing a pelvic mass that subsequently proves to be a malignant ovarian tumor. The reproductive age woman is more likely to have a functional ovarian cyst or endometrioma.
Physical Examination • Perform a comprehensive examination. • Attention to the lymph-node-bearing areas • Particularly the supraclavicular and inguinal areas. • Examination of the abdomen • Abdominal distention • The presence of flank fullness and shifting dullness • Tympanitic percussion note over the lateral abdomen a large mass displacing the bowel to the periphery. • central tympanitic percussion note ascites
Characteristics of a pelvic mass on physical examination BENIGN !! Mobile Cystic Unilateral Cul-de-sac: smooth MALIGNANT !! Fixed Solid or form Bilateral Cul-de-sac:nodular
Radiographic Evaluation-I • Ultrasonography • Transabdominal • Transvaginal • Color flow doppler studies • CT retroperitoneal structures,pelvic organs • MRI more information regarding the nature of the ovarian tumor. • High cost and questionable benefit !!! • Particular benefit in the evaluation of pregnant woman.
Radiographic Evaluation-II • Radiograph of the chest exclude metastatic parenchymal disease and detect pleural effusion. • Barium enema • Screening mammogram study
Radiographic characteristics that help to differentiate benign and malignant adnexal masses BENIGN *Simple cyst, <10 cm in size *Septations, <3 mm in thickness *Unilateral *Calcification, especially teeth *Gravity-dependent layering of cyst contents MALIGNANT *Solid or cystic+solid *multiple septations >3mm in size *bilateral *ascites
PROGNOSTIC FACTORS • Stage !! • Grade • Cell-type of tumor • Residual disease aftersurgery • Disease volume prior to any surgical debulking • Age of woman >70 • Performance status
SCREENING FOR OVARIAN CANCER NO EVIDENCE THAT SCREENING WORKS!! • Ultrasound • Transvaginal • Abdominal • Color flow • Tumor Markers: • Ca 125 • Protein patterns • Pelvic exam • Genetic screening
SURGICAL TREATMENT of epithelial overian cancer • Surgery:the cornerstone of therapy • debulking: • remove as much ofthe cancer as possible • the less cancer leftafter primary surgerythe better theoutcome • the best outcome iswhen there is noresidual disease
At the time of diagnosis, >70% of patients with epithelial ovarian cancer have metastases beyond the pelvis • . The most common locations of metastases: *peritoneum (85%) *omentum (70%) *liver (35%) *pleura (33%) *lung (25%) *bone (15%) Lymphatic metastasis occurs frequently, with up to 80% involving pelvic lymph nodes and 67% involving para-aortic lymph nodes, depending on the stage of cancer.