Download

1 / 14
140 likes | 283 Views
From Peer to Infinity. Engaging Peers as Partners in Needle Exchange. Private sector training, consultancy and research service run by and for people who use drugs. Team’s unique selling point is its dual professional and experiential expertise.

E N D
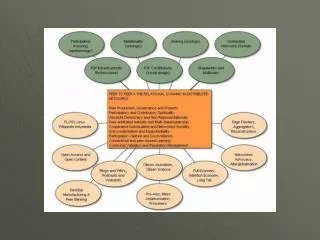
From Peer to Infinity Engaging Peers as Partners in Needle Exchange
Private sector training, consultancy and research service run by and for people who use drugs. Team’s unique selling point is its dual professional and experiential expertise. Special focus on emerging drug trends. GST plays a role described by Dr Sloboda from NIDA as bridge-building – fostering communication and learning between academic, practice and using communities. Mat Southwell & Tam Miller AKA: Mr White & Mr Brown
Overview • Deploying peer-based needle exchange as an integral part of harm reduction services – a drug service manager’s view – Mat Southwell • From underground peer needle exchange to professional partnerships – the drug user group experience – Tam Miller • From demons to angels – the role of drug dealers in delivering peer needle exchange – Nikki Coe
The East London Experience - Context • 1989 (HOT founded in 1991) • High levels of poverty & 40% black & minority ethnic communities • High drug prevalence exacerbated through housing policies • 5% HIV rates but migrant trends from Latin EU Countries, Scotland and Ireland • Very under-developed services in late 1980s – mostly medical drug dependency units and no community services • Emergence of new drug trends
The East London Experience – Interventions • Healthy Options Team employed community harm reduction model – organisational culture consistent • Peer volunteering in needle exchange • Formalised secondary needle exchange – reaching female heroin using mothers, emerging injectors in BME communities, recreational gay dance drug users, etc • Community outreach and peer support re: new drug trends • Harm reduction innovation – RTIs, crack, viral protection campaign
The East London Experience - Lessons • Merits of whole system, strategic approach to community harm reduction including employment of people who used drugs • Rapid growth and investment in services from Regional AIDS Funding supported innovation • Engagement with European models (i.e. Mainline) supported engagement with international standards of community involvement • Challenges of championing community models given resistance in field and lack of understanding among commissioners • Partnership and fostering of drug user organising
The Niddrie Experience - Context • From 1986 • High levels of concentrated poverty - Edinburgh’s poorest scheme • High prevalence of injecting, particularly Temgesic (low dose buprenorphine), heroin and benzos • 50% HIV rates reflecting police restrictions on injecting supplies in 1980s and pattern of group sharing • At time services very limited and based in city centre and only during office hours. Needle exchange bus didn’t arrive until 1992
The Niddrie Experience - Interventions • Informal sourcing of sterile injecting equipment – ‘peer sharing’ • Illegal needle exchange – home and community based – operating within Niddrie • Mutual aid formalised with launch of Chemical Reaction user group in 1993 with Issues of Substance magazine • User group chair employed as Drugs Development Worker for Castle Project between 1995 to 2002 • Return to informal needle exchange after service relationship ends
The Niddrie Experience - Lessons • Ability of people who use drugs and their organisations to respond to community-level threats with or without drug services • Partnerships with drug services sustained while they are effective – partnership working is not a goal in and of itself but can be helpful • Privileged-access into closed drug scene • Working in a ‘deep community’ – reach and impact • Informal secondary exchange continues but reduced conversation with drug services
The North East Essex Experience - Context • Mid-1990s • Heroin and amphetamine sulphate main drugs of choice with strong injecting profile • Semi-rural area providing barriers to service engagement for people who inject drugs in the villages and towns around Colchester and Clacton • Very conservative drug treatment system – poor access and retention • Outreach service run from Health Promotion with clear community philosophy
The North East Essex Experience - Interventions • Volunteers recruited from peer and ‘straight’ communities • Key success of programme was its engagement of local drug suppliers as secondary needle exchange providers • Training provided from Healthy Options Team • Volunteer supervision • Independent researcher evaluates impact and reach of scheme – Annette Walling • Voice of Independent Drugusers (VOID) launched and self-funded magazine
The North East Essex Experience - Lessons • Outreach worker left and service incorporated back into drug treatment system resulting the abandonment of community model and secondary needle exchange scheme • Evaluation of model provided important evidence lacking from previous 2 examples – showed enduring impact • Innovation possible when service held in compatible management environment but failure to take wider system with community models is weakness of project • Dealing network targeted by police and many secondary supplies imprisoned for up to five years
Peer Needle Exchange - Shared Lessons • Merits of secondary needle exchange in ‘closed’ drug scenes • Ability of peer needle exchanges to reach cultural sub-groups who may be out of contact with services • Particular benefits of reaching women who injected drugs • Engaged with trends and risk behaviour at coal face supports work around harm reduction innovation • Positive focus for work of drug user groups • Sustained involvement of peers beyond formal service