Download
1 / 37
370 likes | 483 Views
The Cracked Heart: the cardiac effects of cocaine. Denise Watt Nov. 6, 2008. Case. 22 male Found confused, agitated by mom 4g cocaine day prior + 4g today Combative with EMS, 10mg midazolam IM PMHx: smoker, asthma, polysubstance abuse Meds: ventolin, flovent. Case.

E N D
The Cracked Heart: the cardiac effects of cocaine Denise Watt Nov. 6, 2008
Case • 22 male • Found confused, agitated by mom • 4g cocaine day prior + 4g today • Combative with EMS, 10mg midazolam IM • PMHx: smoker, asthma, polysubstance abuse • Meds: ventolin, flovent
Case • 36.5, 180, 60, 88P, 100%, 3.8 • Diaphoretic, agitated • GCS 11, PERLA 4mm • CV/CNS nil
Case cont. • Bolus NS, Midazolam • ABG: 7.30/30/106/14 • Agitated, GCS 9 • Intubated • ?seizure Ativan • Labs: • Cr 164, CK 500/MB 60, TnT 0.07 • AG 20, urine +ve cocaine, cannabis
Case cont • CCU consulted • Fluids, Ativan • Extubated 5 hr later – admit CCU • Peak TnT 0.12, CK 14000, LDH >2500 • Resting Echo: • low normal LV fn • upper normal size • Transfer to IM • Uneventful course
Outline • Overview of cocaine • Cardiac effects • Cocaine-associated chest pain • Diagnosis • MI • Management • Controversies • Beyond the ED
Coca • Coca plant leaves • South America ≥ 1200 years • CNS stimulant, anesthetic • Medicalized 1800s • Controlled 1970 • “epidemic” late 1980s • 2nd most common illicit drug • 14% have used (US 2003) • Crime • Highest drug-related offenses in Calgary Source: Wikipedia
Street forms • Cocaine • Hydrochloride salt • IV, snort • Blow, C, marching powder, nose candy • Crack • Alkaloid (free base) • add NaHCO3 rock • smoke cracks • Freebase, rooster, tornado Source: Wikipedia
Pharmacology • NE/Epi/Dopamine/serotonin re-uptake inhibitor • Na+ channel blocker • Metabolism: hepatic urine metabolites • Peak onset • Seconds inhaled,1-2min IV, 15-30min nasal • Duration • 5-10min inhale, 15-30min IV, 1 hr nasal • t½: 1hr • Metabolites up to 8 hr • Urine metabolites 4 – 72 hr • Cocaine + ETOH cocaethylene
Desired Effects • Euphoria • Increased energy “You perceive an increase of self-control and possess more vitality and capacity for work.... Long intensive physical work is performed without any fatigue...This result is enjoyed without any of the unpleasant after-effects that follow exhilaration brought about by alcohol” -Sigmund Freud Wikipedia
Non-cardiac Effects • CNS stimulant • agitation, hallucinations, psychosis, seizures, ICH, CVA • Muscle activity • Rhabdomyolysis, hyperthermia • Anesthetic • Appetite suppressant • Vascular • HTN, Aortic dissection • Highly addictive, tolerance
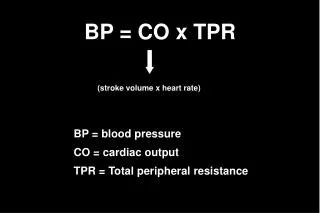
Cardiac effects:acute • HR, BP, contractility • Coronary vasoconstriction • Thrombosis • Arrhythmias oxygen demand + oxygen supply = ischemia
Cardiac effects:chronic • Accelerated atherosclerosis • HTN • LVH • Systolic dysfunction • Cardiomyopathy • Myocarditis
Cocaine-associated chest pain • CP most frequent ED presentation • “Typical” pt: young, male, smoker DDx: • Cardiac: ischemia/MI • MSK: rhabdo, trauma • Pulmonary: barotrauma, “crack lung” • Aortic dissection
Cocaine-associated MI (CAMI) • 6% CP1 • Younger, fewer RF • ¼ non-fatal MIs young patients • 20-50% no CAD • Highest risk in 1st hour2 • 24 times baseline • up to 4 days • No predictors of CAMI, TIMI not predictive3 • In-hospital mortality low • High incidence recurrent events 1. Hollander J. Prospective Multicenter Evaluation of Cocaine-associated Chest Pain. Acad Emerg Med. 1994;1:330-339 2. Mittleman M. Triggering of Myocardial Infarction by Cocaine. Circulation. 1999;99:2737-2741 3. Chase . Application of the TIMI risk score in ED patients with cocaine-associated chest pain. Am J Emerg Med 2007;25:1015-1018
History Ask! Timing of use, route, amount, regular use PE Signs of acute toxicity ECG Non-sensitive Non-specific 43% have STE BER, LVH Labs AG/ABG, LFTs, Cr, CK, urine Mb CKMB non-specific Urine drug screen? Chest pain approach
Case 27yo male presents with Lt chest tightness, diaphoresis, tachycardia, hypertension. ECG/CXR normal. Smoker. Denies cocaine/drugs. RN states anxious. Do you: • use Guantanamo-style interrogation • give him Ativan and send home • do a urine drug screen
Urine drug screening • No studies • Widely used in US • Why? • Initiate drug counseling • May change management • Why not? • Low yield • Takes hour(s) • Usefulin some situations • Young, few RF, high suspicion ACS, MI • Toxic-appearing
Management of cocaine-associated chest pain • Benzodiazepines (I/B) • Animal studies • Decreases central stimulatory effects decreases CV effects • RCT • Relieves CP • Decreases HR, BP • May be only agent needed • ASA (I/C) • Nitrates (I/B) • 2 RCTs • Relieves CP, reverses coronary VC, decreases BP
BZD vs. NTG • Small DBRCT diazepam vs. NTG vs. diazepam + NTG • 40 pt with ischemic-sounding CP • Outcomes: cardiac performance (impedance), hemodynamic, CP • 3 MI, 5 USA • No differences Bottom line: use either If CNS effects present, use BZD Baumann B. Randomized, double-blind, placebo-controlled trial of Diazepam, Nitroglycerin, or both for treatment of patients with potential cocaine-associated acute coronary syndromes. Acad Emerg Med. 2000;7:878-885
Management of CACP • CCB (IIb/C) • Unclear benefit • If no response to BZD/NTG • Phentolamine (IIb/C) • Cath lab study, animal models • Reverses coronary vasoconstriction • HCO3 • Ventricular arrhythmias • B-blockers??
Β-blockers in CACP • Contraindicated due to unopposed alpha • Lange et al3 • 30 volunteers elective cath for chest pain work-up • Intranasal cocaine vs. placebo • Intracoronary propanolol vs. placebo • Cocaine: coronary vasoconstriction • Worsened by propanolol • Esmolol, labetolol – mixed results • AHA III/C 3. Lange R. Potentiation of Cocaine-induced coronary vasoconstriction by Beta-adrenergic blockade. Annals of Int Med. 1990;112:897-903
B-blocker controversy • Cocaine-associated MI ≠ vasospasm • Thrombosis major cause • 80% of CAMI had significant CAD4 • Benefits of B-blockers • decrease O2 demand • prevent re-infarction and arrhythmias 4. Kontos M. Coronary angiographic findings in patients with cocaine-associated chest pain. J Emerg Med. 2002;24:9-13.
Dattilo et al. 2008 • Retrospective cohort study • Telemetry/CCU/ICU admits with +ve urine cocaine
Dattilo et al. • 6% MI after B-blocker • 26% not receiving B-blocker had MI • B-blocker reduced risk of MI (OR 0.06) • No significant mortality difference • Suggest protective effects out ways potential harm
Limitations • Retrospective, small • Patient population • ICU/CCU/telemetry admission • ½ patients had CP • No data on time of ingestion • ?effect after acute ingestion • No B-blocker group sicker? • most deaths due to sepsis • Benefit in ACS is long term use
B-Blockers + cocaineBottom Line • No great studies • Effect in acute cocaine ingestion unknown • Likely harmful • Possible long term benefit • AHA 2008: consider post-discharge in: • LV dysfunction, ventricular arrhythmias • BUT high recidivism • No role in the ED
Thrombolytics in cocaine-associated STEMI • No studies showing efficacy • Mortality CAMI low • Poor specificity ECG • ?Safety • risk ICH • Risks of lytics out way benefits • Use PCI if clear STEMI
Case cont. Patient finally admits to smoking crack 2 x week. Pain-free post Ativan. What now?
Chest pain unit • Prospective, cohort study • 302 moderate-low risk patients with CACP • Observed 6-12 hr, serial ECG + TnT • 158 stress test • 4 positive (3%) 3 positive angiograms • 30 day outcome: 4 MI • All continued to use cocaine, ≥ 2 RF • No deaths • AHA recommends observe x 9-12 hr • Stress testing “optional” Weber J. Validation of a brief observation period for patients with cocaine-associated chest pain. N Engl J Med. 2003;348:510-7
Risk Stratification • Myocardial perfusion imaging • 1 study, 216 patients • 100% sensitive for MI • Missed 2 significant CAD • Echocardiography • LVH more common • May mask wall motion abnormalities • Stress testing • Case series 6 pt • + stress tests within 2 weeks post use • 5 no CAD, 1- 70% LM CABG • Repeat cath for recurrent CP – patent LM, diffuse vasospasm • Authors suggest delaying stress test 2-3 weeks post abstinence
Angiography • 90 high risk patients • 34% MI • 77% had significant CAD • 32% 1VD, 10% 2VD, 5.6% 3VD • Selection bias Kontos, M. Coronary Angiographic findings in patients with cocaine-associated chest pain. J Emerg Med 2003;24:9-13
Disposition/Follow-up • CAMI – admit • High risk - admit • Moderate-low risk – observe 9-12 hours • 10hr TnT likely reasonable • Recurrent visits, other risk factors • Out-patient risk stratification • Education • Drug counseling/cessation programs
Take Home Points • Ask about cocaine use in ?ACS patients • MI uncommon, low mortality • Highest risk first hour post ingestion • Treatment: • BZD, ASA, nitrates • Brief observation for moderate-low risk • ?out-patient risk stratification • High risk/MI • Admit, rule out CAD • Drug cessation