Download
1 / 31
330 likes | 416 Views
MR campaign Rationale and overview Dr Vikas Kokare, MPH State Coordinator, WHO, Gujarat. Why MR and not MMR? Why up to 15 years of age? Why campaign, we are already giving it routinely? Why not give it to adolescent girls only?

E N D
MR campaign Rationale and overview Dr Vikas Kokare, MPH State Coordinator, WHO, Gujarat
Why MR and not MMR? • Why up to 15 years of age? • Why campaign, we are already giving it routinely? • Why not give it to adolescent girls only? • Why to give if already taken all recommended doses in RI already?
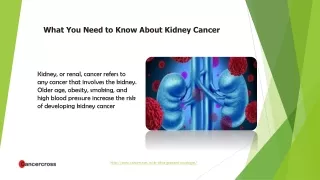
Measles mortality: due to complications Corneal scarring causing blindness Vitamin A deficiency Encephalitis Older children, adults ≈ 0.1% of cases Chronic disability Pneumonia & diarrhea Diarrhea common in developing countries Pneumonia ~ 5-10% of cases, usually bacterial
Rubella and CRS Rubella Congenital Rubella Syndrome Hearing Impairment Cataracts / Glaucoma Heart defects ( PDA ) Microcephaly Developmental Delay Mental retardation Hematological disorder Liver and spleen damage • lymphadenopathy • Arthritis • Children: rare • Adult female: up to 70% • Thrombocytopenic purpura • 1/3000 cases • Encephalitis • 1/6,000 cases
Measles & Rubella outbreaks wide spread, India, 2015-16 2015 2016 Measles Rubella Mixed *: As on March-2017
Measles Mortality in India ~ 36 % in 2014 49,200 out of 134,200 measles deaths globally, (WER No. 45, 2016, 91, 525-536) Measles deaths Dots are randomly distributed in countries
CRS sentinel surveillance sites by ICMR • Six sites operational: • AIIMS, Jodhpur • CMC, Vellore • IGICH, Bengaluru • KEM, Pune • PGIMER, Chandigarh • TMH, Jamshedpur ICMR, DELHI Proposed 20 surveillance sites NIE, CHENNAI NIV, PUNE
Estimates of the median incidence of CRS per 100,000 live births by country in 2010 Estimated – 40-50 thousand cases of CRS annually in India Vynnycky E et al. (2016) Using Seroprevalence and Immunisation Coverage Data to Estimate the Global Burden of Congenital Rubella Syndrome, 1996-2010: A Systematic Review. PLoS ONE 11(3): e0149160.
To summarize • Mumps is not a disease of public health importance compared to other competing priorities. • Adding Mumps component doubles the cost of vaccine. • So it is like spending twice as much money and with no significant benefits in terms of decrease in disease morbidity and mortality particularly < 5 mortality. • Besides that money can be used in prevention of other diseases of public health importance like Diarrhea, Pneumonia by introducing RVV, PCV.
Age distribution of Measles cases - India, 2015-16* (> 90% of cases are under 15 years of age) Vaccinated Not Vaccinated Unknown 2016 2015 • ~ 95% Measles < 15 years of age • ~ 96% Measles < 15 years of age 44% 35% 39% 38% 8% 8% 11% 7% 4% 5% Total cases- 17,198 Total cases- 30,606 (Cases from serologically confirmed measles outbreaks only) *: as on March-2017
Age distribution of Rubella cases – India (2015-2016*) (> 90% of cases are under 15 years of age) * data as on July 2016
3. Why campaign, why not jut introduce it in routine immunization ?
Measles Mortality in India ~ 36 % in 2014 49,200 out of 134,200 measles deaths globally, (WER No. 45, 2016, 91, 525-536) Measles deaths Dots are randomly distributed in countries
Vaccination status of Measles cases in the country 2015 2016 Total cases- 30,606 Total cases- 17,198 80% of the measles cases are unvaccinated , reflecting Wide immunization gap in the country
Currently national MCV1 coverage is 65 % (NFHS4). MCV 2 will be lesser than this (target is > 95% coverage for both). • And as can be seen, there is wide immunization gap. • If we wait for RI coverage to reach 95% for both (MCV1 & 2), it will take few more years. • During this period we will loose many more infants & <5 children due to Measles related complications (and we already bearing 1/3 of the global death burden) • And all these deaths are preventable • And way to quickly bridge this immunization gap & boost population immunity is through campaign
Age distribution of Rubella cases – India (2015-2016*) (> 90% of cases are under 15 years of age) * data as on July 2016
Reasons for campaign mode • Age shift – virus moving in higher age group leading to higher cases of CRS after vaccine introduction (Paradoxical effect) • Therefore boosting population immunity up to 15 years of age population before Rubella vaccine introduction is essential. • And the way to achieve this in short period of time again is through a campaign.
Measles Immunization Campaign, 2011 to 2012 BAN PAT KTC SBK MSN GNC PML GNR AMC KDA DHD SRN RJT AND VDC AMD JMD RJC JMC BVC VDD NMD BRH BVN AML POR JUC SRC SRT TAP JUN DNG NAV VLD Phase 1, Mar to Jul 2011 Phase 2, Jan 12 to Mar 2012 Phase 3, Sep 12 to Dec 2012
Measles Outbreaks in 2010 (before the Campaign) BAN PAT KTC SBK MSN GNC PML GNR AMC KDA DHD SRN RJT AND VDC AMD JMD RJC JMC BVC VDD NMD BRH BVN AML POR JUC SRC SRT TAP JUN DNG NAV VLD N = 33 Lab confirmed Measles Outbreaks
Measles Outbreaks in 2013 (after the Campaign) BAN PAT KTC SBK MSN GNC PML GNR AMC KDA DHD SRN RJT AND VDC AMD JMD RJC JMC BVC VDD NMD BRH BVN AML POR JUC SRC SRT TAP JUN DNG NAV VLD N = 7 Lab confirmed Measles Outbreaks
Post campaign building of susceptible cohort State wide Measles Campaign 2011-12 *Data source – WHO SIMS data *Data as of Week No.52, ending of 31/12/2017
Why not just give Rubella vaccine to the adolescent girls only ?
Operationally very challenging to achieve high coverage (>95%) in adolescent girls leading to suboptimal coverage. • Besides the active virus transmission still remains in the community (in boys). • Sub-optimal coverage plus easy virus availability (from boys) continues to have CRS cases thus leading to failure of CRS prevention. • This strategy has failed in the past in places like Kerala and some Corporations
Why to give MR vaccine even if the child has received all the recommended doses of Measles/MMR in RI ?
Vaccine failure • Primary vaccine failure: This is when a person fails to produce antibodies (at detectable levels) or does not produce enough antibodies considered necessary to protect from the disease. • Secondary vaccine failure: This is when a person does produce antibodies in response to vaccination however the levels wane and decline at a faster rate than normally expected. However, antibodies to almost all vaccines decline over time, even after booster shots.
Vaccination status of Measles cases in the country 2015 2016 Total cases- 30,606 Total cases- 17,198 ~ 80 of the measles cases are unvaccinated , reflecting Wide immunization gap in the country
Vaccine failure continues….. • In some children protective antibodies do not develop even after 2 doses of measles vaccine (vaccine efficacy is 85% < 1 yr and 95% > 1 yr) • In very small fraction of sero-converted children, antibody titers wane over a period of time (immunological memory loss) • Secondary vaccine failure in outbreaks of disease amongst the vaccinated is frequent.