Download
1 / 34
380 likes | 743 Views
ULCERATIVE COLITIS. Dr.Mohammadzadeh. Research shows that close to 70 percent of people who have active UC in a given year will have a relapse of symptoms in the next year . A large part of treating UC is preventing the next relapse and keeping it in remission as much as possible.

E N D
ULCERATIVE COLITIS Dr.Mohammadzadeh
Research shows that close to 70 percent of people who have active UC in a given year will have a relapse of symptoms in the next year. • A large part of treating UC is preventing the next relapse and keeping it in remission as much as possible. • When there is a flare, management aims to relieve symptoms and end the flare-up as soon as possible.
What is a UC flare? • A UC flare refers to a worsening of the symptoms of bowel inflammation. It’s marked by disabling symptoms, such as:
Moderate to severe abdominal pain or cramps that aren’t helped by ordinary pain or antispasmodic medications • Bleedingfrom the rectum or blood in the stool • Moderate to severe diarrhea that may lead to dehydration in severe cases • Weight loss due to loss of appetite and diarrheal symptoms • Inability to have a satisfactory bowel movement • Nutritional issues resulting from frequent and severe flaring
What are the common triggers of UC? • Every person with UC has different triggers. Next slideis a list of some of the most common triggers:
Certain medications - broad-spectrum antibiotics - nonsteroidal anti-inflammatory drugs and other painkillers • Abrupt withdrawal from medications can also lead to a flare especially steroids. • Younger people have a higher risk of flares.
Changes in the level of hormones during pregnancy can cause a relapse of symptoms or acute flares. • Any condition or infection that alters electrolyte levels in the body can also induce a flare. This includes diarrhea from any infectious or noninfectious cause, like traveler’s diarrhea.
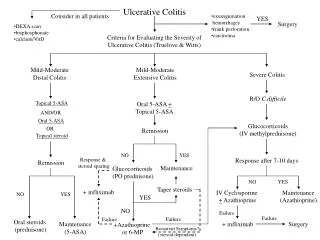
Dealing with flares • Steroids: These can be given systemically (either by mouth or intravenously) or as enemas. • 5-Aminosalicylates: This medication gets released in different parts of the gastrointestinal tract depending upon the medicine. • Immunomodulators: These include medications such as azathioprine or methotrexate. They work on the immunologic system. • Antibiotics: These are used because infections often contribute to flares. • Biologics: These work on the immune system too and include infliximab (Remicade), adalimumab(Humira), and certolizumab (Cimzia)
FULMINANT ULCERATIVE COLITIS • Fulminant colitis refers to a subgroup of patients with severe ulcerative colitis who have more than 10 stools per day, continuous bleeding, abdominal pain, distension, and acute, severe toxic symptoms including fever and anorexia. • Such patients are at risk of progressing to toxic megacolon and bowel perforation
Initial therapy • Patients with fulminant colitis should be admitted to a hospital and followed closely with vital signs and physical examination every four to six hours to evaluate abdominal and rebound tenderness and more frequently if there is clinical deterioration. • Stool output should be recorded to chart the number and character of bowel movements, including the presence or absence of blood and liquid versus solid stool.
A complete blood count, serum electrolytes, serum albumin, liver function tests, and erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) should be checked every 12 to 24 hours and more frequently if there is clinical deterioration.
Intravenous fluid and electrolyte replacement are necessary to correct and prevent dehydration or electrolyte imbalance. Blood transfusions may be needed to maintain a hemoglobin ≥10 g/dL.
Patients with intestinal dilation (transverse colon diameter ≥5.5 cm) should receive decompression with a nasoenteric tube. Intermittent rolling maneuvers every two hours or the knee-elbow position should be recommended to help redistribute gas in the colon and thereby promote decompression .
Plain abdominal radiography should be repeated if there is clinical deterioration to determine if there is colonic dilation (diameter ≥5.5 cm) or toxic megacolon (diameter ≥6 cm or cecum >9 cm and systemic toxicity).
Patients with fulminant colitis should be treated with intravenous glucocorticoids. Prednisolone (30 mg IV every 12 hours) or methylprednisolone (16 to 20 mg IV every eight hours) are preferred because they produce less sodium-retention and potassium-wasting. • All patients with fulminant disease should be treated with broad-spectrum antibiotics • All patients should receive pharmacological venous thromboembolism prophylaxis
Subsequent therapy • Patients with fulminant ulcerative colitis who fail to improve by the third day of intensive treatment should be managed as patients with steroid-refractory ulcerative colitis with eithercyclosporine or infliximab, or undergo colectomy. • However, the threshold to undergo colectomy in patients who fail to respond to cyclosporine or infliximab is lower.
Colectomy Patients with fulminant colitis who fail treatment with cyclosporine or infliximab (either due to a failure to respond or due to relapse) within four to seven days and those with toxic megacolon (diameter ≥6 cm or cecum >9 cm and systemic toxicity) who do not respond to therapy within 72 hours, require colectomy.