Download
1 / 34
340 likes | 467 Views
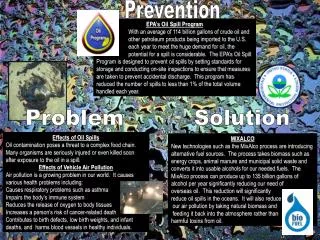
Prevention. Prevention Track. Rapporteur Team: Rene Ekpini (Rapporteur) Edward Bitarakwate Irene Benech Shanti Conly Beverly Cummings Mary Fanning Rachel King Jan Moore John Pitman Caroline Ryan. Outline. The principle of knowing your epidemic and knowing your response

E N D
Prevention Track Rapporteur Team: Rene Ekpini (Rapporteur) Edward Bitarakwate Irene Benech Shanti Conly Beverly Cummings Mary Fanning Rachel King Jan Moore John Pitman Caroline Ryan Prevention Rapporteur Presentation
Outline • The principle of knowing your epidemic and knowing your response • Most at risk populations • Addressing multiple and concurrent partnerships • Broadening the array of prevention service providers • Military response to the HIV epidemic • Prevention with PLWH • Prevention of mothers-to-child transmission • Key messages and conclusion Prevention Rapporteur Presentation
Generalized vs concentrated epidemics • There is no “global epidemic”—but a multitude of epidemics • Generalized and concentrated epidemics are fundamentally different in who gets infected and how • In the Americas, Europe, Asia and the Near East HIV has spread in one or more defined subpopulation and not well established in the general population and will probably always remain concentrated • We need to better understand the mixed epidemics in the Caribbean, W. Africa, Papua and elsewhere Prevention Rapporteur Presentation
The response • Concentrated HIV epidemics can be prevented, stabilized and reversed • But in the face of challenging environments, MSM and IDU programs have not fully developed or gone to scale • In generalized epidemics, countries have been slow to respond to the drivers, including lack of male circumcision and multiple concurrent partnerships Prevention Rapporteur Presentation
Are programmes reaching the most vulnerable, at-risk and underserved populations? Are they providing services appropriate to the population in an appropriate way? Can these be brought to scale? Providing the right response Prevention Rapporteur Presentation 7 June 2008
In Rwanda, a multi-sectoral committee ensures that refugees can access the full range of HIV services in a camp ( #679 ) In Kenya, a National Technical Working Group on Drug-users, Injecting drug-users and Prisoners coordinates provision of HIV and drug related services (# 751) In South Africa, outreach to sex workers is provided through brothel based services ( #1560 ) In Russia, demand for risk reduction and HIV, STI and TB services increased through case workers and training to reduce discrimination by medical professionals ( #774) Linking vulnerable populations to comprehensive responses Prevention Rapporteur Presentation 7 June 2008
Mass media with community mobilization and interpersonal communication Special programs and curricula for FBOs/CBOs Integration into existing programs Prevention outreach with peer education PMTCT HIV Counseling and testing (especially couples testing) Life Skills Programs Models for Reducing Concurrent Partnerships Cote d’Ivoire
WHO/UNAIDS Technical Consultation, Montreux, March 2007 Recommendation 1.1: Male circumcision should now be recognized as an efficacious intervention for HIV prevention Recommendation 2.1: Male circumcision should never replace other known methods of HIV prevention and should always be considered as part of a comprehensive HIV prevention package Male circumcision in the context of PMTCT Neonatal circumcision Circumcision of male partners Recommendations
Swaziland, Zambia most advanced; can share experience ( #1688; #1754; #1844) MC recommended for HIV-negative men Complication rates low for trained medical providers, higher for traditional providers but need to find ways to involve them Need to mobilize political support for scaling-up Consider task shifting due to human resource constraints Scaling up with quality for population-level impact Lessons learned
MC should be part of comprehensive prevention package HIV testing and counselling Active exclusion of symptomatic STIs and syndromic treatment where required Provision and promotion of male and female condoms Counselling on risk reduction and safer sex Surgical procedures performed as described in the WHOManual for Male Circumcision under Local Anaesthesia Post-op follow-up and ongoing risk reduction counselling Minimum package for MC services
Programme experience: actors and approaches • Peer educators or mentor mothers (Mothers2Mothers): • Field Officers training local residents to provide comprehensive behaviour change counselling to their community (Total Control of the Epidemic – TCE) • Training of Clients to serve others – Aroma therapists, Community ART Support Agents, Front Desk office, Drama groups, Palliative, Care workers (TASO) • Training of FBO and church leaders to conduct participatory workshops, deliver sermons, and provide peer support and counselling to church members on mutual monogamy and HIV prevention
Military response to HIV/AIDS Understanding the enemy [HIV] terrain and counterattacking
Best practice prevention in military and peacekeeping operations in Benin, Lesotho and Uganda • Strategic framework developed for military prevention • Behavioral and serological surveillance • Openness about prevalence in the armed forces • Comprehensive, decentralized approach to prevention pre, post and during deployment, including mobile testing • Peacekeeping (PKO) pay after post-deployment health check • Issue: is exclusion of PLWHA from PKO discriminatory? Prevention Rapporteur Presentation
Poster promoting condom use Addressing vulnerability Poster promoting abstinence of youngpeople
“Ma vie, Ma decision”: a mass media campaign - Cote d’Ivoire addressing gender norms and HIV prevention among youth Youth living on the street – Kenya Link with authorities, services to meet special needs, e.g., food security, livelihood Integrate with regular youth activities Increase self-esteem, return to school and employment (#845) Adolescent girls living in slums – Ethiopia Door to door recruitment; good reach to most vulnerable Mentor – peer educator, ensure follow-up Group participation including literacy, life skills, HIV education, GBV, psychosocial support (#1094) Accessing hard to reach youth
Need more involvement of people living with HIV in development and implementation of prevention programmes (#1356) Need for programmers to understand experience of people with HIV to develop meaningful prevention programs ( #594) Integration of prevention into HIV care and treatment needs to be accelerated Targeted messages on: sexual prevention of HIV; disclosure; discordant couples; family planning; stigma and discrimination
Impact of increased emphasis on Blood Safety • HIV prevention funding from PEPFAR strengthens Guyana’s ability to effectively manage a limited supply of safe blood for transfusion (Abstr 988) • Impact of awareness of Injection Safety – • In Haiti, training and awareness campaigns ensure private sector buy-in and support for a new law requiring the exclusive importation and use of auto-disable (AD) syringes (Abstr 178) • In Kenya, collaboration and awareness-building with medical training school faculty and other medical curriculum stakeholders leads to growing acceptance of injection safety as a necessary element in medical school training (Abstr 1905)
Percentage of HIV positive pregnant women receiving ARVs for PMTCT, by region, 2004-2007
In South Africa and LesothoHAART in pregnant women was feasible, safe and effective with lower infection rates among infants whose mothers received treatment in South Africa – 0.3% (Abst 938) and Lesotho-2.0% (Abst 959) In Malawi, Rwanda and Mozambiqueaccess to CD4, reorganization of services and mentoring clinical staff significantly increased the number of eligible women enrolled for ARV prophylaxis and ART for their own health . Moving toward more efficacious ARV regimens including ART for PMTCT Insert Title: Prevention, Treatment, etc. Rapporteur Presentation 7 June 2008
In Zambia HIV testing and counseling in labor ward of women with unknown HIV status increased population coverage by 16% (312) Increase in uptake of services improvement of facilities, quality control and community-based interventions including involvement of male partners in Tanzania (425) CD4 cell count and linkages with ART center supported by monitoring, community mobilization, peer support groups and provision of delivery packsin Nigeria (487) Outreach ANC/PMTCT with linkage to ART clinic for CD4and ART for populations with low access to facility-based ANC in Ethiopia Increasing access and uptake through innovations
Exclusive breastfeeding up to 6 months carries a lower risk of HIV transmission than mixed feeding (South Africa) Breast feeding promotion on scale is possible as evidenced by improvements in Madagascar, Bolivia and Ghana ( Abst. 1776) Exclusive breastfeeding rate improved from less than 5 percent in 1992 to 56 percent in 2004 in Malawi and from 26 percent in 1996 to 40 percent in 2001/2002 in Zambia In Uganda HIV free survival did not differ by feeding option (formula 76.6%, breast feeding 75.3%) however 12 month mortality was significantly higher in the formula fed group (Abst. 1898) Infant feeding counselling and support
Successful prevention programme requires good knowledge of drivers of the epidemics • “When you know the enemy and how he operates, you know how to respond”-(President Museveni—A1 Opening Ceremony) • Ensure synergies between prevention, treatment, care and support programes • Optimize funding by selecting the appropriate interventions • Ensure that programmes reach the most vulnerable, at-risk and underserved populations: MSM, IDUs, SWs • Specific intervention to address multiple concurrent partnerships • Address vulnerability of young people Prevention Rapporteur Presentation
There is no one magic bullet – need multiple component prevention package combining behavioural, structural and biomedical interventions Broaden the array of prevention service providers PMTCT should in the first place prevent new infections among women of childbearing age and increase access to more efficacious ARV regimens including ART for pregnant women in need of treatment PMTCT should go beyond infections averted and deliver on the goal of improved maternal and child health and survival Prevention Rapporteur Presentation 7 June 2008
Scaling up through partnerships: time for contribution and not attribution PEPFAR WHO UNICEF