Download
1 / 27
270 likes | 382 Views
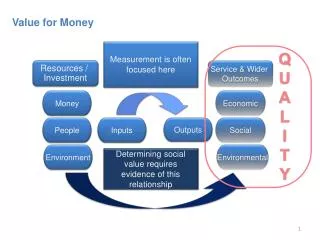
Value for money How to design RCTs to ensure their compatibility with economic evaluation. Kevin Marsh. September 2006. Introduction and overview. Question : what are the methodological lessons from attempts to build economic evaluations on RCTs?. Source of evidence

E N D
Value for moneyHow to design RCTs to ensure their compatibility with economic evaluation Kevin Marsh September 2006
Introduction and overview • Question: • what are the methodological lessons from attempts to build economic evaluations on RCTs? • Source of evidence • two recent NICE public health reviews • Challenges • measuring the cost of interventions • standardised measure of effects • generalising 2 requests 1 question
Why are we concerned with value for money? Campbell Collaboration Economic Methods Group (CCEMG) Policy Brief (in press): Provision of evidence on cost-effectiveness, alongside evidence on the benefits and adverse effects of interventions, can significantly enhance […] decision-making by managers and policy makers.
effectiveness -ve +ve y x Effectiveness plane • Should we invest in intervention ‘x’? • yes – ‘x’ is more effective than ‘y’ • but what is the opportunity cost of ‘x’?
Cost-effectiveness plane +ve effectiveness -ve y +ve cost -ve
Cost-effectiveness plane +ve • Should we invest in ‘x’? • yes - ‘x’ dominates ‘y’ effectiveness -ve y +ve cost -ve
Cost-effectiveness plane +ve • Should we invest in ‘x’? • no - ‘y’ dominates ‘x’ -ve y +ve effectiveness cost -ve
Cost-effectiveness plane +ve effectiveness -ve y +ve • Should we invest in ‘x’? • ? – cost-effect trade off? cost -ve
Aren’t we already doing economic evaluation? Number of studies identified in 2 recent reviews of effectiveness and economic studies
Intervention risk factor (e.g. cigarette use) probability substance misuse probability problematic SM health, crime, unemploy. £ pp £ saved pp QALY gain pp How do we model value for money from RCTs?
Intervention risk factor (e.g. cigarette use) probability substance misuse Cost / risk factor probability problematic SM health, crime, unemploy. £ pp £ saved pp QALY gain pp (£ pp- £ saved pp) / QALY gained pp How do we model value for money from RCTs?
Intervention risk factor (e.g. cigarette use) probability substance misuse Review of effectiveness (RCT) probability problematic SM health, crime, unemploy. £ pp £ saved pp QALY gain pp How do we model value for money from RCTs?
Intervention risk factor (e.g. cigarette use) probability substance misuse Step 1: cost intervention? probability problematic SM health, crime, unemploy. £ pp £ saved pp QALY gain pp How do we model value for money from RCTs?
Good description of a simple intervention • Facilitate referral to an external treatment agency • discuss negative consequences of personal drug use • discuss impediments to reducing negative consequences • advice about appropriate services • discuss possible impediments to treatment • arrange the first appointment with a named counselor • reminder telephone call prior to the first appointment • offer of transport to first appointment • offer to accompany then to their first appointment
Example: intervention description • Facilitate referral to an external treatment agency • discuss negative consequences of personal drug use • discuss impediments to reducing negative consequences • advice about appropriate services • discuss possible impediments to treatment • arrange the first appointment with a named counselor • reminder telephone call prior to the first appointment • offer of transport to first appointment • offer to accompany then to their first appointment 1. Who provides the intervention?
Example: intervention description • Facilitate referral to an external treatment agency • discuss negative consequences of personal drug use • discuss impediments to reducing negative consequences • advice about appropriate services • discuss possible impediments to treatment • arrange the first appointment with a named counselor • reminder telephone call prior to the first appointment • offer of transport to first appointment • offer to accompany then to their first appointment 2. How long does each element take?
Example: intervention description • Facilitate referral to an external treatment agency • discuss negative consequences of personal drug use • discuss impediments to reducing negative consequences • advice about appropriate services • discuss possible impediments to treatment • arrange the first appointment with a named counselor • reminder telephone call prior to the first appointment • offer of transport to first appointment • offer to accompany then to their first appointment 3. % take up optional elements?
Request 1: resource use data • describe resource use: who does what, what equipment? • measure resource use: hours, units? • value resource use: £
Intervention risk factor (e.g. cigarette use) probability substance misuse probability problematic SM health, crime, unemploy. £ pp £ saved pp QALY gain pp How do we model value for money from RCTs? Step 2: CE?
Step 2: calculating cost-effectiveness Intervention 1: Cost - £100 Effect – YP not use cannabis in last month when would otherwise Intervention 2: Cost - £100 Effect – YP move from use cannabis 20 times/yr to only 5 times/yr
Intervention risk factor (e.g. cigarette use) probability substance misuse probability problematic SM health, crime, unemploy. £ pp £ saved pp QALY gain pp How do we model value for money from RCTs? Step 3: long-term effect?
Same risk factors Different measures E.g. Use cannabis in the last month? Y/N Use cannabis > 31 times/yr? Y/N ? Step 3: modelling long-term effect RCT: Change in YP risk factors Epidemiological: Impact risk factors on LR sub. misuse
NICE econ review: matching effect studies to epidemiological data 6 only model fraction of the effects identified
Request 2: use standard measures of effect • compare between studies • link with epidemiological data
How generalisable are our results? • RCTs: conflicting + inconsistent results • Heterogeneity
If yes Alternative method? Quasi-exp? Other? RCT for each combination of intervention, control, population, context? Question: how do we overcome the challenge of heterogeneity? Can an RCT only tell us about intervention X if implemented in way A, for population B, in social context C?