Download
1 / 48
490 likes | 768 Views
Visual Inspection with Acetic Acid (VIA) for Skin Cancer. Presented by Davidson KE, Teeter KA and Young KE. BIO 4410 November 22, 2011. Introduction. Developing countries are lacking the resources needed for qualitative health care. Introduction.

E N D
Visual Inspection with Acetic Acid (VIA)for Skin Cancer Presented by Davidson KE, Teeter KA and Young KE BIO 4410 November 22, 2011
Introduction • Developing countries are lacking the resources needed for qualitative health care
Introduction • Developing countries are lacking the resources needed for qualitative health care • Patients need to be diagnosed early enough to prevent expensive surgery and potentially death
Introduction • Developing countries are lacking the resources needed for qualitative health care • Patients need to be diagnosed early enough to prevent expensive surgery and potentially death • Our biotechnology includes Visual Inspection with acetic acid (VIA) to detect skin cancer
Health Insurance and Spending • Health Spending has been focused on developing countries because: • Increase in higher disease rates • Lack of resources • Limited health care providers • Competition for necessary health care
Health Insurance and Spending • Health Spending has been focused on developing countries because: • Increase in higher disease rates • Lack of resources • Limited health care providers • Competition for necessary health care • Global spending on health totaled to approximately 2.3 trillion dollars
Health Insurance and Spending • Health Spending has been focused on developing countries because: • Increase in higher disease rates • Lack of resources • Limited health care providers • Competition for necessary health care • Global spending on health totaled to approximately 2.3 trillion dollars • Developing countries account for 84% of the population
Health Insurance and Spending • Health Spending has been focused on developing countries because: • Increase in higher disease rates • Lack of resources • Limited health care providers • Competition for necessary health care • Global spending on health totaled to approximately 2.3 trillion dollars • Developing countries account for 84% of the population • Even though the health debate has been focusing on developing countries, 50 million Americans also do not have health insurance, while 25 million are underinsured.
Skin Cancer Worldwide • Skin cancer is the most common cancer worldwide • Researchers are trying to find a more effective way to diagnose and treat skin cancer in poor regions, such as Brazil http://www.mnn.com/health/fitness-well-being/stories/outbreak-of-deadly-infection-in-brazil-worries-officials
3 Most Common Skin Cancers • The skin is composed of three layers, any of which can become cancerous • Squamous Cell Carcinoma (SCC) • Basal Cell Carcinoma (BCC) • Malignant Melanoma (MM) • These skin cancers have low mortality rates, but can lead to serious surgery if not treated in time http://ocaesthetics.org/dermal-medical-skin-care-oc-aesthetics-medical-group-ca.html
Squamous Cell Carcinoma (SCC) • The top layer of the skin contains squamous cells • Cancer of these cells is called squamous cell carcinoma (SCC) • Caused by x-ray exposures, burns, and chemical damage. • Approximately accounts for 16% of skin cancers. http://trialx.com/curetalk/2011/02/squamous-cell-clinical-trials-treatments-research-centers/
Basal Cell Carcinoma (BCC) • Second layer of skin comprised of basal cells • Cancer of these cells is called basal cell carcinoma (BCC) • Caused by sun exposure • Mostly found on head and neck • Makes up 80% of skin cancer • Most common form of skin cancer http://www.veteranstoday.com/2011/06/06/basal-cell-and-squamous-cell-skin-carcionmas/
Occurs in the deepest (third) layer of the skin called melanocytes Melanocytes produces melanin, which gives the skin color Melanoma is the most lethal form of skin cancer Malignant Melanoma (MM) http://cancer.osu.edu/patientsandvisitors/cancerinfo/cancertypes/skin/about/melanoma/pages/index.aspx http://bryanking.net/warning-signs-of-malignant-melanoma/
http://www.health.ny.gov/statistics/diseases/cancer/skin/report/2010/http://www.health.ny.gov/statistics/diseases/cancer/skin/report/2010/ Pie Chart on SCC, BCC, Malignant Melanoma, and Other Skin Cancers
Skin Cancer in Developing Countries, such as Brazil • The Brazilian National Cancer Institute (INCA) estimates that for 2010, there will be: • 119,780 new cases of non melanoma and • 5,930 new cases of melanoma skin cancer • The 5- year survival rate for patients with melanoma • In developed countries is 73% • In developing countries is 56% • Survival rate reflects delayed diagnosis
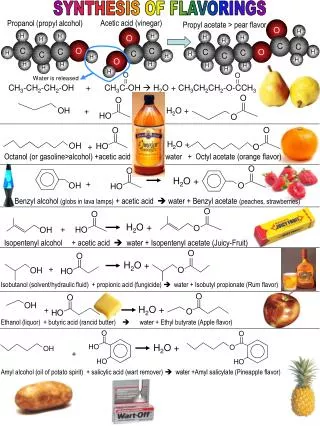
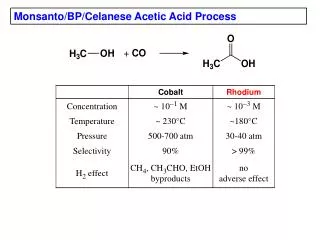
Supporting Research, Part I (Cervical Cancer) • Identified the role of acetic acid in cervical cancer screening in developing countries • Cervical cancer is a type of SCC • Acetowhite lesions are visible with the naked eye one minute after application of acetic acid • More severe forms of cancer retain acetowhite effect longer (5-10 minutes) than less severe forms http://www.wpclipart.com/medical/doctor_equipment/Disposable_medical_nitrile_glove.png.html
Sensitivity verses Specificity • Sensitivity = # true positives (# true positives + # false positives) • Specificity = # true negatives (# true negatives + # false negatives) • Visual inspection screening (VIA) using 3%-5% acetic acid • Sensitivity: 61%, Standard Deviation: 0.12 • Specificity: 69%, Standard Deviation: 0.056
Supporting Research, Part I (Continued) Figure 1: Lucianiet al.VIA(+) test results according to agein TATI-2 study
Supporting Research, Part II (Skin Cancer) • Use VIA to perform a non-invasive diagnosis of the following: • Squamous cell carcinoma (SCC) • Basal cell carcinoma (BCC) • Malignant melanoma (MM) • Goal: to differentiate cancerous lesions from normal skin cells and benign lesions such as: • Epidermal keratinocytes • Pigmented nevi • Seborrheickeratoses • Potential for false positives: • Callus • Wart • Eczema http://www.bobthepharmacist.com/practical-health-care/was-it-a-mole-a-wart-or-a-basal-cell-skin-cancer
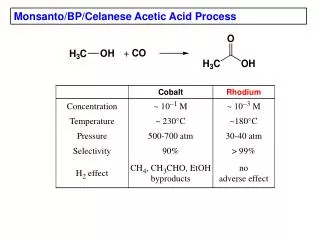
Supporting Research, Part II (Continued) • Figure 2: Patel et al. Excised BCC samples (5-6μm thick) after exposure to 3% acetic acid for 1 min • Lower concentrations of 1%-3% acetic acid are better when used in direct contact with living skin tissue • High concentrations of 5%-10% acetic acid are better when used on skin excisions
Proposal Conclusion • Use of VIA protocol to be tested as a method to enable the rapid in vivo confirmation of abnormal (precancerous or cancerous) tissue
Proposal Conclusion • Use of VIA protocol to be tested as a method to enable the rapid in vivo confirmation of abnormal (precancerous or cancerous) tissue • After completing checklist of exlusionary conditions, a solution of 3% acetic acid would be applied to the suspect tissue • A second coat is to be applied after two minutes
Proposal Conclusion • Use of VIA protocol to be tested as a method to enable the rapid in vivo confirmation of abnormal (precancerous or cancerous) tissue • After completing checklist of exlusionary conditions, a solution of 3% acetic acid would be applied to the suspect tissue • A second coat is to be applied after two minutes • Any tissue that demonstrates acetowhitening is to be removed
Current Diagnosis Methods • Begins with a visual examination by a doctor using the AABCD rule http://topnews.us/content/239336-brooklyn-college-holds-melanoma-awareness-event
Current Diagnosis Methods • Begins with a visual examination by a doctor using the AABCD rule • Asymmetry: one section of the skin growth is different in size or shape than the other section http://www.skinsight.com/info/health_article/2008/05/15/may-skin-cancer-awareness
Current Diagnosis Methods • Begins with a visual examination by a doctor using the AABCD rule • Asymmetry: one section of the skin growth is different in size or shape than the other section • Any skin growth that bleeds or will not heal http://www.revolutionhealth.com/conditions/cancer/skin-cancer-melanoma/special-feature
Current Diagnosis Methods • Begins with a visual examination by a doctor using the AABCD rule • Asymmetry: one section of the skin growth is different in size or shape than the other section • Any skin growth that bleeds or will not heal • Borders: irregular borders http://healthknowitall.net/health-care/2009/05/20/summer-time-increases-risk-of-skin-cancer/#more-911
Current Diagnosis Methods • Begins with a visual examination by a doctor using the AABCD rule • Asymmetry: one section of the skin growth is different in size or shape than the other section • Any skin growth that bleeds or will not heal • Borders: irregular borders • Color: color varies from one area to another: tan, brown, black, red, bluish or pale white http://healthknowitall.net/health-care/2009/05/20/summer-time-increases-risk-of-skin-cancer/#more-911
Current Diagnosis Methods • Begins with a visual examination by a doctor using the AABCD rule • Asymmetry: one section of the skin growth is different in size or shape than the other section • Any skin growth that bleeds or will not heal • Borders: irregular borders • Color: color varies from one area to another: tan, brown, black, red, bluish or pale white • Diameter: larger than 6 mm in size (think of the size of a pencil eraser)
http://www.northcoastfootcareblog.com/may-is-skin-cancer-awareness-month/http://www.northcoastfootcareblog.com/may-is-skin-cancer-awareness-month/
Confirmation of Diagnosis • Requires biopsy • Sample examined under a light microscope http://www.microscope-manufacturers.com/compound-light-microscope.html
Degree of Accuracy by DoctorInitial Visual Examination Helfand 2001
Degree of Accuracy by DoctorInitial Visual Examination Helfand 2001
Degree of Accuracy by DoctorInitial Visual Examination Helfand 2001
Biopsies Performed Per Malignancy Helfand 2001
Other Proposed Options http://www.einstein.yu.edu/aif/instructions/aobs/index.htm http://rozeklaw.com/whiplash-neck-injury.htm
VIA Comparability • VIA accuracy comparable to a primary care physician http://216.30.190.224/search/searchAMResultImg.aspx?searchStr=adenosquamous+carcinoma+of+cervix&rootTerm=squamous+cell+carcinoma+of+cervix&searchType=1&rootID=40893 http://www.physiciansnews.com/2010/11/29/docs-should-screen-younger-patients-for-eating-disorders/
VIA Compared to Biopsies • No excision • No risk of infection • 10 minutes to identify lesion • Lower emotional toll to patient VIA Biopsy Requires excision Risk of infection Several days to identify lesion Higher emotional toll to patient http://www.fastmoleremoval.com/surgical-mole-removal http://health.lifegoesstrong.com/put-down-q-tip
VIA Compared to Biopsies • No expensive equipment • No electricity • No trained technician • Portable VIA Biopsy Expensive equipment Electricity Trained technician Not portable http://www.fastmoleremoval.com/surgical-mole-removal http://health.lifegoesstrong.com/put-down-q-tip http://www.avantgarde-metal.com/content/beyond2.php?id=60
VIA Benefits - Miscellaneous • Non toxic • Even cheaper if combined with other diagnostics http://www.testpaternity.co.uk/dna-testing-kit/ http://www.sciencephoto.com/media/295305/enlarge
Current Diagnostic Methods are Costly http://www.electricitysuppliers.com/98/ugi-electric-company/ http://www.orionhsv.com/medicalstaffing.html http://www.diylife.com/2008/01/02/10-clever-ways-to-conserve-water/ http://topnews.ae/content/28963-new-medicine-reference-formulae-be-given-out-soon http://www.altiusdirectory.com/Gallery/album.php?n=Currencies-&albumid=162&id=1520 http://www.microscope-manufacturers.com/compound-light-microscope.html
VIA is Cost Effective + = http://www.kids-pages.com/folders/colpages/Jobs/page14.htm http://technorati.com/business/finance/article/vinegar-putting-basics-to-use-in/
Collins SR, Kriss JL, Doty MM, Rustgi SD. 2008. Losing Ground: How the Loss of Adequate Health Insurance Is Burdening Working Families—Findings from the Commonwealth Fund Biennial Health Insurance Surveys, 2001–2007. The Commonwealth Fund 99. • Drezek RA, Collier T, Brookner CK, Malpica A, Lotan R, Richards-Kortum RR, Follen M. 2000. Laser scanning confocal microscopy of cervical tissue before and after application of acetic acid. American Journal of Obstetrics and Gynecology 182(5): 1135-1139. • Ekalaksananan T, Pientong C, Thinkhamrop J, Kongyingyoes B, Evans MF, Chaiwongkot A. 2010. Cervical cancer screening in north east Thailand using the visual inspection with acetic acid (VIA) test and its relationship to high-risk human papillomavirus (HR-HPV) status. Journal of Obstatrics and Gynaecology Research 36(5): 1037-1043. • Ferris DG, Cox JT, O’Connor DM, Wright VC, Foerster J. 2004. Modern colposcopy: Textbook and atlas. ASCCP . 2nd ed: 197. • Gaffikin L, McGrath JA, Arbyn M, Blumenthal P. 2007. Visual inspection with acetic acid as a cervical cancer test: accuracy validated using latent class analysis. BioMed Central Medical Research Methodology 7(36): 1-10. • Gallagher RP. 2005. Sunscreens in melanoma and skin cancer prevention. CMAJ 173(3): 244-245. • Gniadecka M, Philipsen PA, Sigurdsson S, Wessel S, Nielsen OF, Christensen DH, Hercogova J, Rossen K, Thomsen HK, Gniadecki R, Hansen LK, and Wulf HC. 2004. Melanoma Diagnosis by Raman Spectroscopy and Neural Networks: Structure Alterations in Proteins and Lipids in Intact Cancer Tissue. The Society for Investigative Dermatology, Inc. 122(2): 443-449. • Helfand M, Mahon SM, Eden KB, Frame PS, Orleans, CT. 2001. Screening for Skin Cancer. American Journal of Preventive Medicine 20(3,1): 47-58, • INCA 2002. Prevenção do Câncer de pele. Rev Bras Cancerol 48(3): 317-332. • Luciani S, Munoz S, Gonzales M, Delgado JM, Valcarcel M. 2011. Effectiveness of cervical cancer screening using visual inspection with acetic acid in Peru. International Journal of Gynecology and Obstetrics 115(1): 53-56. • MacLean AB. 2004. Acetowhite epithelium. Gynecologic Oncology 95(3): 691-694. • Nora AB, Panarotto D, Lovatto L, Boniatti MM. 2004. Frequency of counseling for skin cancer prevention by the various specialties in Caxias do Sul.An bras Dermatol 79(1): 45-51. • Patel YG, Nehal KS, Aranda I, Li Y, Halpern AC, Rajadhyaksha M. 2007.Confocal reflectance mosaicing of basal cell carcinomas in Mohs surgical skin excisions. Journal of Biomedical Optics 12(3): 1-10. • Quentin W, ADu-Sarkodie Y, Terris-Presholt F, LegoodR, Opoku BK, Mayaud P. 2011. Costs of cervical cancer screening and treatment using visual inspection with acetic acid (VIA) and cryotherapy in Ghana: the importance of scale. Tropical Medicine & International Health 16(3): 379-389. • SBD (SociedadeBrasileira de Dermatologia) 2003.Perfil dos dermatologistas no Brasil: Relatório final (Brasil e grandesRegiões). In EscolaNacional de SaúdePública . Edited by FundaçãoOswaldo Cruz, p38. • Uliasz A, Lebwohl M. 2007. Patient education and regular surveillance results in earlier diagnosis of second primary melanoma.Int J Dermatol 46(6): 575-577.