Download
1 / 15
150 likes | 282 Views
Matrix 2. Ukeme A. Udoh University of the District of Columbia. HEALTH DISPARITY IN SMOKING TOBACCO. Can hospitals stop their Employees and patient and visitors from smoking anywhere?. OBJECTIVES. Discuss the health hazards associated with smoking

E N D
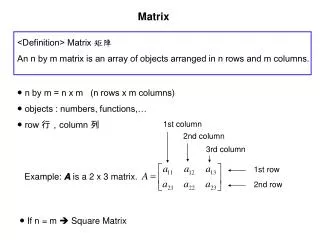
Matrix 2 Ukeme A. Udoh University of the District of Columbia
HEALTH DISPARITY IN SMOKING TOBACCO Can hospitals stop their Employees and patient and visitors from smoking anywhere?
OBJECTIVES Discuss the health hazards associated with smoking To review and discuss effect of smoke free policies within the health care facility. Statistical data from smoke related deaths Show a clinical proposal to evaluate tobacco use and tool to prevent smoking Articulate goals and objectives of the selected tool Provide rationale for the choice of tool
INTRODUCTION • Smoking tobacco is a national health epidemic that claims the lives of many individuals annually (American lung association,2012) • This is particularly alarming due to the preventable nature of smoking • While many individuals who smoke have expressed the desire to quit, only a few percent who attempt to stop without a formal intervention
LITERATURE REVIEW Literature 1. Smoke free policies have a cumulative effect on smoking behavior (Berg et al, 2012) Literature 2: A campus wide smoke-free policy has no detrimental effect on measures of employee or consumer attitudes / behaviors (Christine et al, 2009) Literature 3: Smoke free policies around the hospital property have consequences, support for withdrawal important (Annette et al, 2011) Literature 4: Smoke bans reduce employee tobacco use (Wheeler, 2007) Literature 5: State legislation do play a positive role in facilitating health related policy change (knudsen,2010)
A WELLNESS PHILOSOPHY • To assist people to lead meaningful lives in their communities, we need to promote behaviors that lead to good health (primary prevention)
TOBACCO’S DEADLY TOLL More deaths are caused each year by tobacco use than by all deaths from human immunodeficiency virus (HIV), illegal drug use, alcohol use, motor vehicle injuries, suicides, and murders combined 435,000 deaths in the US/year 4.8 million deaths worldwide/year 10 million annual death estimated by 2030 50,000 annual deaths in the US due to second hand smoke exposure (Tobacco-Related Mortality, 2011)
TOOL A: NICOTINE DEPENDENCE • 1. How many cigarettes a day do you usually smoke? • [ ] 1 - 10 0 points • [ ] 11 – 20 1 points • [ ] 21 – 30 2 points • [ ] 31 or more 3 points • 2. What type do you smoke? 0 points • [ ] Low nicotine (0.9 mg or less) 1 point • [ ] Medium nicotine (1.0 – 1.2 mg) 2 points • [ ] High nicotine (1.3 mg or more) 3 points • 3. How often do you inhale the smoke from your cigarette? • [ ] Never 0 points • [ ] Sometimes 1 points • [ ] Always 2 points • 4. How soon after you wake up do you smoke your first cigarette? • [ ] Within less than 5 minutes 3 points • [ ] Within 6-30 minutes 2 points • [ ] Within 31-60 minutes 1 points • 5. Do you smoke more during the first two hours of the day than during the rest of the day? • [ ] No 0 points • [ ] Yes 1 points • 6. Which cigarette would you most hate to give up? • [ ] The first cigarette in the morning 1 point • [ ] Any cigarette other than the first one 0 points • 7. Do you find it difficult to refrain from smoking in places where it is forbidden, such as public • buildings, on airplanes or at work? • [ ] No 0 points • [ ] Yes 1 point
TOOL B: SELF EVALUATION STAGE • SELF EVALUATION Tobacco Use & Quitting • Please mark the spot that reflects how important it is for you to change your tobacco use? • Not Important Very Important Not Confident Very Confident? • Please mark the point that reflects how confident you are that you can change your tobacco usage. • On the following scale, which point best describes how ready you are at this time to change your tobacco habit?
TOOL C: CLINICAL PROGRAM: EVIDENCE BASED MODEL Ask: Systemically identify all tobacco users Advise: Advise tobacco users to quit Assess: Assess each tobacco users willingness to quit Assist: Assist tobacco users with a quit plan Arrange: Arrange follow-up contact (Jamal et al, 2012)
SHORT TERM GOAL AND OBJECTIVE OF SLECTED PROGRAM • To improve awareness, knowledge and attitudes related to cessation among adult smokers. • To improve awareness, knowledge and attitudes related to cessation among health care system staff, health care professionals and insurance purchaser • Promote decreased social acceptability of tobacco use • Promote health system change
LONG TERM GOAL OF SELECTED PROGRAM Increase the percentage of smokers who intend to quit Decrease smoking rate among pregnant women To Encourage health care providers to counsel patients to quit using tobacco To promote smoke cessation programs in workplaces and other community setting
RATIONALE FOR PROGRAM SELECTED The tool is simple and easy to use It creates a follow up relationship between the physician and patient. As a clinical practice guideline, tool addresses areas and enables the HCP to teach patients on the importance of quitting Consistent use of this tool increases health care provider knowledge and skill in dealing with tobacco dependent adult
References American lung association. (2012). Retrieved from http://www.lung.org /stopsmoking/aboutsmoking/healtheffects/smoking.html Berg, C., Swan, D., Fredrick, G, Daniels, S., & Kegler, M., (2012) Smoke- free Policies at home, church and work: Smoking levels and recent quit attempts among a southern rural population 2007. Prevention chronic disease 1-9 Jamal, A., Dube, S. R., Malarcher, A. M., Shaw, L., & Engstrom, M. C. (2012, june15). Tobacco Use Screening and Counseling During Physician Office Visits Among Adults — National Ambulatory Medical Care Survey and National Health Interview Survey, United Tobacco-Related Mortality. (2011). Retrieved from Center for Disease Control website http://www.cdc.gov/tobacco/data_statistics/fact_sheets/health_effects
References • Annette S.H Schultz, B. F. (2011). A qualitative investigation of smoke free policies on hospital property. CMAj.JAMC, 1-9 • Christine Shaffer, M. S. (2009). Smoke Free Medical Facility Campus Legislation: Support, resistance, difficulties and Cost. International journal of Environmental research and Public Health, 1-6.Incomplete • Hannah k. Knudsen, S. (2010). Substance Abuse Treatment Counselors and Tobacco Use: A Comparison of Comprehensive and Indoor only Workplace Smoking bans. Oxford Journals o Nicotine and Tobacco Research, 1-4 ( Use APA to provide enough information here for the reader to retrieve the source of your entry).(volume, issue) • J Gary wheeler, l. P. (2007). Impact of a Smoke Free hospital Campus Policy on Employee and Consumer Behavior. Public Health Reports, 1-6.