Download
1 / 1
10 likes | 86 Views
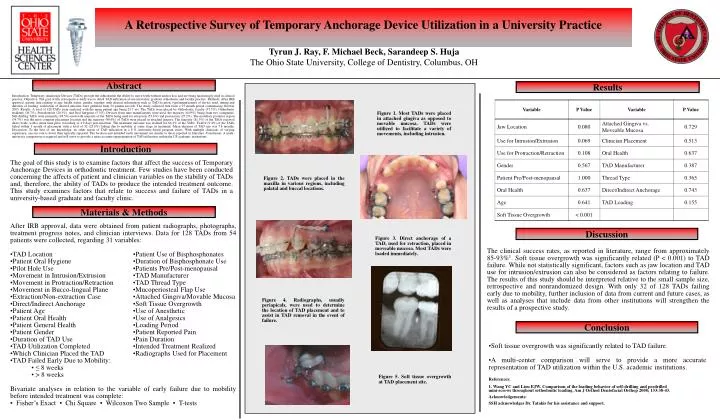
Introduction. Results. Materials & Methods. Abstract. Discussion. Conclusion. A Retrospective Survey of Temporary Anchorage Device Utilization in a University Practice. Tyrun J. Ray, F. Michael Beck, Sarandeep S. Huja The Ohio State University, College of Dentistry, Columbus, OH.

E N D
Introduction Results Materials & Methods Abstract Discussion Conclusion A Retrospective Survey of Temporary Anchorage Device Utilization in a University Practice Tyrun J. Ray, F. Michael Beck, Sarandeep S. Huja The Ohio State University, College of Dentistry, Columbus, OH Introduction: Temporary Anchorage Devices (TADs) provide the orthodontist the ability to move teeth without anchor loss and are being increasingly used in clinical practice. Objective: The goal of this retrospective study was to detail TAD utilization at one university graduate orthodontic and faculty practice. Methods: After IRB approval, patient data relating to age, health status, gender, together with clinical information such as TAD location, type/manufacturer of device used, timing and duration of loading, realization of desired outcome were gathered from 54 patient records. The study collected data from a 35 month period commencing October 2005. Results: A total of 128 TADs were analyzed with the mean patient age being 23.7 yrs. The TADs were placed by Orthodontic faculty (37.5%), Orthodontic residents (36.7%), Periodontists (20.3%), and Oral Surgeons (5.5%). Devices from nine manufactures were used, the majority (64.9%) being from two companies. Self-drilling TADs were primarily (94.5%) used with majority of the TADs being used for retraction (53.6%) and protraction (27.2%). The maxillary posterior region (54.7%) was the most common placement location and the majority (90.6%) of TADs were placed in attached gingiva. The majority (81.3%) of the TADs received direct loads, with a mean time prior to loading of 4.9 days post-insertion. The treatment outcome was realized for 66.4% of the TADs. Twelve (9.4%) of the TADs failed within 1 month of placement with a total of 32 (25.0%) failing due to mobility at some stage in treatment. Mean duration of TAD use was 7.8 months. Discussion: To the best of our knowledge, no other report of TAD utilization in a U.S. university-based program exists. With multiple clinicians of varying experience, success rate is lower than typically reported. The location and intended tooth movement are similar to those reported in literature. Conclusion: A multi-university comparison is required and will serve to provide a more accurate representation of TAD utilization within the US academic institutions. Figure 1. Most TADs were placed in attached gingiva as opposed to movable mucosa. TADs were utilized to facilitate a variety of movements, including intrusion. The goal of this study is to examine factors that affect the success of Temporary Anchorage Devices in orthodontic treatment. Few studies have been conducted concerning the affects of patient and clinician variables on the stability of TADs and, therefore, the ability of TADs to produce the intended treatment outcome. This study examines factors that relate to success and failure of TADs in a university-based graduate and faculty clinic. Figure 2. TADs were placed in the maxilla in various regions, including palatal and buccal locations. After IRB approval, data were obtained from patient radiographs, photographs, treatment progress notes, and clinician interviews. Data for 128 TADs from 54 patients were collected, regarding 31 variables: • TAD Location •Patient Use of Bisphosphonates • Patient Oral Hygiene •Duration of Bisphosphonate Use • Pilot Hole Use •Patients Pre/Post-menopausal • Movement in Intrusion/Extrusion •TAD Manufacturer • Movement in Protraction/Retraction •TAD Thread Type • Movement in Bucco-lingual Plane •Mucoperiosteal Flap Use • Extraction/Non-extraction Case •Attached Gingiva/Movable Mucosa • Direct/Indirect Anchorage •Soft Tissue Overgrowth • Patient Age •Use of Anesthetic • Patient Oral Health •Use of Analgesics • Patient General Health •Loading Period • Patient Gender •Patient Reported Pain • Duration of TAD Use •Pain Duration • TAD Utilization Completed •Intended Treatment Realized • Which Clinician Placed the TAD •Radiographs Used for Placement • TAD Failed Early Due to Mobility: • ≤ 8 weeks • > 8 weeks Bivariate analyses in relation to the variable of early failure due to mobility before intended treatment was complete: ▪ Fisher’s Exact ▪ Chi Square ▪ Wilcoxon Two Sample ▪ T-tests Figure 3. Direct anchorage of a TAD, used for retraction, placed in moveable mucosa. Most TADs were loaded immediately. The clinical success rates, as reported in literature, range from approximately 85-93%1. Soft tissue overgrowth was significantly related (P < 0.001) to TAD failure. While not statistically significant, factors such as jaw location and TAD use for intrusion/extrusion can also be considered as factors relating to failure. The results of this study should be interpreted relative to the small sample size, retrospective and nonrandomized design. With only 32 of 128 TADs failing early due to mobility, further inclusion of data from current and future cases, as well as analyses that include data from other institutions will strengthen the results of a prospective study. Figure 4. Radiographs, usually periapicals, were used to determine the location of TAD placement and to assist in TAD removal in the event of failure. • Soft tissue overgrowth was significantly related to TAD failure. • A multi-center comparison will serve to provide a more accurate representation of TAD utilization within the U.S. academic institutions. Figure 5. Soft tissue overgrowth at TAD placement site. References: 1. Wang YC and Liou EJW. Comparison of the loading behavior of self-drilling and predrilled mini-screws throughout orthodontic loading. Am J Orthod Dentofacial Orthop 2008; 133:38-43. Acknowledgements: SSH acknowledges Dr. Tatakis for his assistance and support.






