Download
1 / 45
460 likes | 653 Views
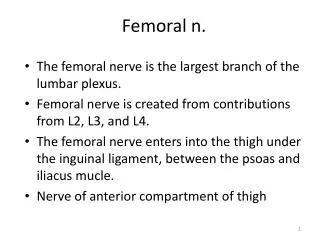
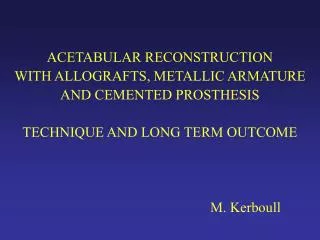
FEMORAL RECONSTRUCTION WITH ALLOGRAFTS. M. Kerboull. Revision with a cemented prosthesis Femoral restoration with allografts Standard femoral component Perfectly suitable to a sound cemented fixation. MAIN SPECIFICATIONS FOR A SOUND CEMENTED PROSTHESIS.

E N D
FEMORAL RECONSTRUCTIONWITH ALLOGRAFTS M. Kerboull
Revision with a cemented prosthesisFemoral restoration with allograftsStandard femoral componentPerfectly suitable to a sound cemented fixation
MAIN SPECIFICATIONSFOR A SOUND CEMENTED PROSTHESIS A polished stem (Ra 0.04 m) ( < 0.1 m ) with a rectangular cross section A tapered shape with a taper angle of 5° Cement and bone subjected only to pressure stresses No shear stresses at the cement bone interface
4 TECHNIQUES Endomedullary reconstruction with impacted cancellous graft Cortical reinforcement with strut grafts Replacement of a destroyed proximal femur with massive allograft Endomedullary reconstruction with a massive femoral graft
ENDOMEDULLARY FEMORAL RECONSTRUCTIONWITH MASSIVE FEMORAL ALLOGRAFT « Double sheath technique »
INDICATIONS • This technique has been used • since 1988 • concurrently with the « impaction grafting » • preferred in cases of severe femoral structural defects • more logical to repair cortical defects with cortical grafts
ITS MAIN INDICATION IS EXTENSIVE OSTEOLYSIS DUE TO AGGRESSIVE GRANULOMATOSIS THAT HAS THINNED DOWN CORTICES WIDENING THE MEDULLARY CANAL AND LOOSENING THE FEMORAL COMPONENT
PRINCIPLES OF THE SURGICAL TECHNIQUE To repair the femoral cortex where it is destroyed, inside the medullary canal, by lining it with a femoral cortical graft
A. After prosthesis and cement removal, reaming and cleaning the medullary canal B. A massive proximal femoral allograft is introduced through the cervical orifice
The graft has to be carrefully shaped so that it excactly and tightly fits the medullary canal all over the extent of the pathologic area without splitting thin cortices Section of the greater trochanter of the graft at the level of the trochanteric osteotomy - obturation of the medullary canal of the graft and host bone by impacted cancellous bone - lining of proximal graft with a strut fragment C. Then a standard femoral component can be cemented into the graft The femoral component is a sheath for the prosthesis and the widened proximal part of the femur a sheath for the graft. This technique requires a bone bank well supplied with proximal femoral allografts. This is relatively rare, and the main limitation of the procedure is the difficulty finding a suitable graft.
Some examples to illustrate this technique
DUR. 06.96 04.95 Loosening of a rough titanium stem Bone restoration with a massive graft
ALB. 09.98 10.98 Loosening of the matte stem with femoral osteolysis Bone reconstruction
BEA. 05.98 03.97 Femoral restoration 1 y. PO A big matte stem
De.G.R. 11.97 09.97 Another case of femoral loosening with osteolysis Double sheath technique 2 months. PO
GAR. 09.99 12.99 Cement bone loosening of a big matte titanium stem Bone restoration with Massive intra medullary allograft 3 months PO
ROB. 09.93 06.91 Major destruction of femoral cortices Bone restoration with massive graft and strut graft
ROB. 09.98 09.98 Lateral view Same case. 7 y. PO AP view
03.98 03.03 10.99 Double sheath technique Using a 250 mm stem and a long graft Extremely severe cortical bone loss X-rays 5 y. PO
BEG. 03.98 03.98 Restoration with massive graft and a 200 mm stem Lateral diaphysal cortical defect
BEG. (2 y. PO) 07.00 07.00 At 2 y. PO excellent bone union between graft and host bone
BEG. 12.02 12.02 03.98 07.00 Same case AP radiograph 5 y. PO
9 years PO AP view Excellent function 2007
GRO. 07.88 09.88 Reconstruction with massive intra medullary graft Loosening of the femoral component
GRO. 2 y. PO 1 m. PO Radiological bone union between the graft on host femoral cortices has been regularly obtained within a year after surgery. Demarcation between graft on host bone visible in the immediate postoperative time has progressively diasappeared, the gap being filled with new bone.
GRO. 03.99 03.99 Same case 11 y. PO. We can hardly distinguish the graft from the host bone
JAN. 03.91 02.98 Another case, radiological result at 7 y. PO
JAN. 07.02 And at 11 y. PO
TRA. 02.89 05.88 The first case operated on in 1988 with the double sheath technique
TRA. 01.99 (10 y. PO) 02.02 (13 y. PO)
X-rays 22 y. PO 2010
MATERIAL 17 WOMEN 9 MEN Average age 67 y. (53 to 83) Operated on from 1988 to 2000 27 femoral reconstructions associated with 24 acetabular reconstructions CHARNLEY-KERBOULL PROSTHESIS 22 Standard 5 Long stem (200 to 250 mm)
MATERIAL PRIMARY DIAGNOSIS 25 coxarthrosis 16 primary 9 secondary 1 osteonecrosis 1 rheumatoid arthritis
MATERIAL PREVIOUS FAILURE OF THR Average 2,1 (1 to 8) LOOSENINGS : - Femoral 27 (mechanical 24, septic 3) - Acetabular 24 (mechanical 21, septic 3)
SOFCOT TYPE III 17 TYPE IV 10 AAOS TYPE III 27 Level II 9 Level III 18 FEMORAL DEFICIENCIES CLASSIFICATION
FOLLOW-UPPhysical and radiological examination at 6 w., 3 m., 1 y. and then every one or two years. AVERAGE FOLLOW-UP 9 y. (3 to 22 y.) LOST 0 DECEASED 4 (5 hips) between 2 and 6 y. PO
COMPLICATIONS 3 NON UNION OF THE GREATER TROCHANTER 2 revised, 1united LATE DISLOCATION 1 FEMORAL FRACTURE (at 2 y.) united after plating 1 FATIGUE FRACTURE OF THE FEMUR (1 y. PO) spontaneously united
BER. 10.97 (8 m. PO) 02.97
BER. (11 m. PO) 01.98 01.98
BER. 11.98 03.03 This fracture spontaneously united X-rays 6 y. PO
CLINICAL RESULTS (d’Aubigné score) PAIN 3 5.9 MOTION 5.2 5.8 STABILITY AND WALKING 3.4 5.6 GLOBAL FUNCTION 11.6 17.4 EXCELLENT (18) 18 VERY GOOD (17) 5 GOOD (16) 1 FAIR (15) 2 POOR (14) 1 23
RADIOLOGICAL RESULTS SUCCESSES 25 Graft host-bone union No loosening No resorption of the graft No subsidence of the graft POTENTIAL FAILURE 1 Partial resorption of the graft No loosening ACTUAL FAILURE 1 Partial resorption of the graft Femoral loosening Not revised
LOZ. 06.90 03.91 Reccurent loosening due to chronic infection. Femoral reconstruction with massive intra medullary graft Early (9 months) resorption of the graft and loosening of the stem
LOZ. 05.94 (4 y. PO) 11.97 (7 y. PO) He couldn’t be reoperated on because of poor cardiovascular conditions
Despite this failure, this reconstruction procedure seems to be valuable and reliable enough to allow us to extend this short series.