Download
1 / 27
270 likes | 283 Views
Explore the role of serotonin in mood regulation, genetics, and stress hormones, while analyzing serotonin and norepinephrine hypotheses in treatment of mood disorders. Discover how neurotransmitters impact emotions and behaviors.

E N D
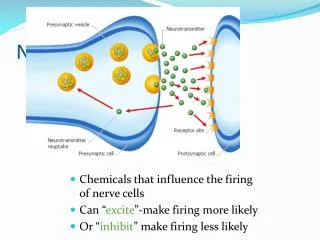
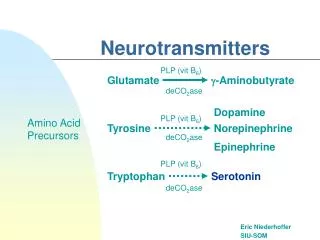
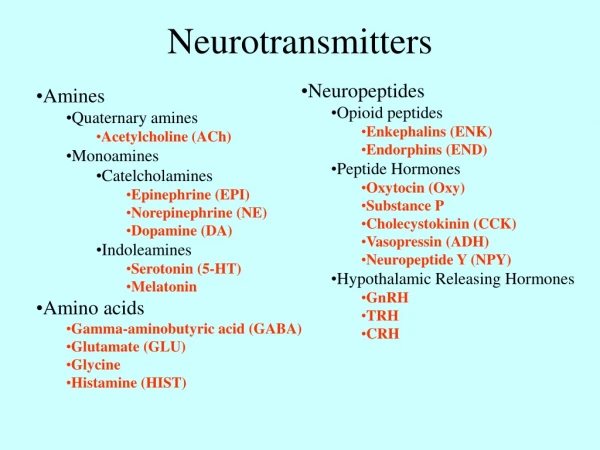
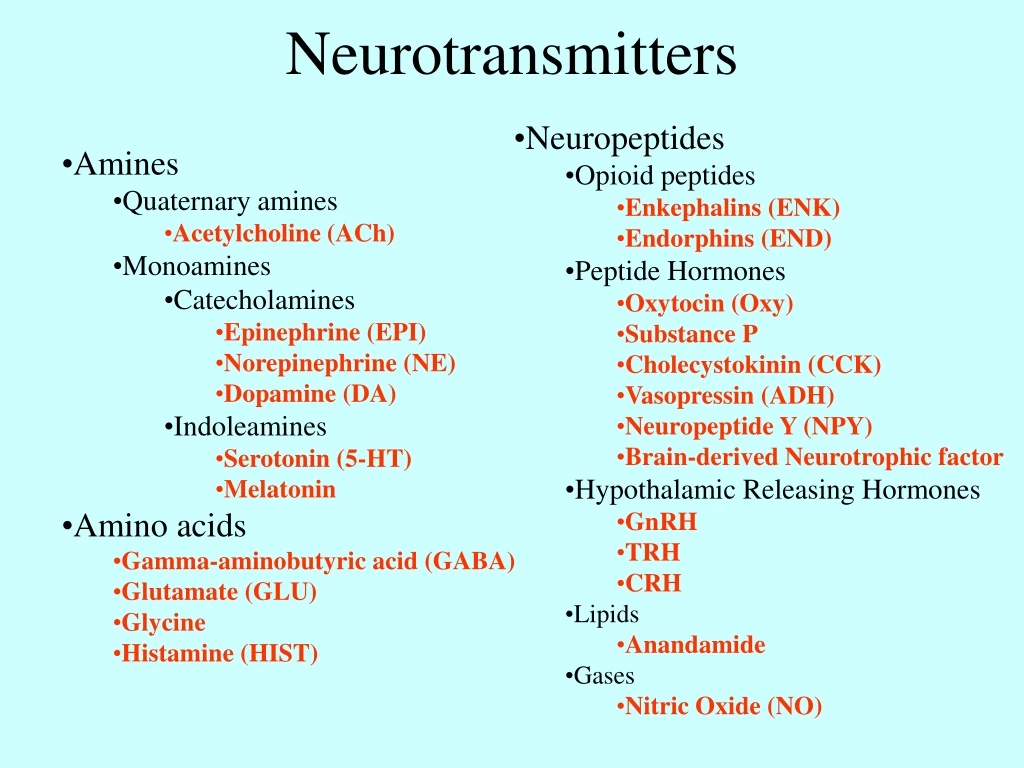
Neurotransmitters • Neuropeptides • Opioid peptides • Enkephalins (ENK) • Endorphins (END) • Peptide Hormones • Oxytocin (Oxy) • Substance P • Cholecystokinin (CCK) • Vasopressin (ADH) • Neuropeptide Y (NPY) • Brain-derived Neurotrophic factor • Hypothalamic Releasing Hormones • GnRH • TRH • CRH • Lipids • Anandamide • Gases • Nitric Oxide (NO) • Amines • Quaternary amines • Acetylcholine (ACh) • Monoamines • Catecholamines • Epinephrine (EPI) • Norepinephrine (NE) • Dopamine (DA) • Indoleamines • Serotonin (5-HT) • Melatonin • Amino acids • Gamma-aminobutyric acid (GABA) • Glutamate (GLU) • Glycine • Histamine (HIST)
5-HT1A-F receptors • CNS • Blood Vessels • 5-HT2A-C receptors • CNS • PNS • Blood Vessels • GI Tract • 5-HT3 receptors • CNS • PNS • GI Tract • 5-HT4 receptors • CNS • PNS • GI Tract • 5-HT5A-B receptors • CNS • 5-HT6 receptors • CNS • 5-HT7 receptors • CNS • Blood Vessels • GI Tract Serotonergic Receptors • Iontotropic • Metabotropic 5-HT1B receptor
5-HT1A and 5-HT2A receptors operate through different signaling mechanisms
Unipolar Disorder (2 wks to 9 mos) • Major Depressive Disorder, Single Episode (MDDSE) • rare • Major Depressive Disorder, Recurrent (MDDR) • family history is common • Dysthymic Disorder (DD) • milder symptoms • chronic occurrence (2-30yrs) • Double Depression • combination or MDDR and DD • Bipolar Disorder (2 wks to 9 mos) • Bipolar I Disorder • Bipolar II Disorder (hypomania) • Dysphoric Mania • manic episodes with simultaneous depression • Cyclothymic Disorder (mild bipolar) Mood Disorders
Major Depressive Episode Characteristics • Onset is in early to mid 20’s • but not age specific • Onset age has been dropping • 16% of population experience • MDD in their lifetime • 2:1 women to men ratio • 41% occurs just before or just • after menstruation
Depression and Stress Hormones • cortisol • steroid hormone
HPA Axis • Hypothalamus • CRF/CRH • Pituitary • ACTH • Adrenals • Cortisol
Stress Diathesis Model • Existing Correlations: • Adult Depression : Elevated Cortisol levels • Childhood Abuse : Adult Depression • Stress Diathesis Model: • Genetic Predisposition plus • Early Abuse/Neglect leads to • Adult Depression • Animal Model shows: • More CRF neurons • Larger CRF neurons • More sensitive CRF neurons • Early abuse permanently alters the stress • response increasing the risk of depression
Monoamine Hypothesis • Originated with observation of Reserpine action: • Inhibits vesicular uptake • Allowing MAO degradation • Reduces levels of DA, NE, and 5-HT • Induces depression-like symptoms • MAOi suppresses depression-like symptoms
Serotonin Hypothesis • Acute Effects: • Transporters blocked • Autoreceptors activated • Cancelling effect • Chronic Effects: • Transporters blocked • Autoreceptors down regulated • Increased 5-HT in synapse
Serotonin Hypothesis • Metabolite of 5-HT: • 5-HIAA • Increased levels found in people who committed suicide
Serotonin Hypothesis • 5-HT Receptors • Less sensitive • Sensitivity restored with use of antidepressants • 5 HT2 Receptors • Increased density • Due to low 5-HT levels? • Chronic use of antidepressants down regulated 5-HT2 receptors
Serotonin-Norepinephrine Hypothesis • down-regulation of β-receptors with chronic antidepressant treatment. • takes 7 to 21 days of treatment, a lag that parallels the onset of therapeutic response in depressed patients. • Similar results occur with many different antidepressants. • But not all antidepressants reduce β-receptors. • There are anatomical and functional interactions between NE neurons originating in the locus coeruleus and the 5-HT neurons in the raphe nuclei. • Each system is capable of modulating the other.
Glucocorticoid Hypothesis • focuses on the stress-related neuroendocrine abnormalities of depression. • Depressed patients have abnormally high CRF secretion. • The hypothalamic CRF neurons are normally controlled by other areas: the amygdala stimulates and the hippocampus has inhibitory control. • When stress is prolonged and intense, glucocorticoid levels remain high, hippocampal neurons are damaged and no longer respond. • Damage includes decreased dendritic branches and spines in the PFC and hippocampus. Formation of new hippocampal cells is inhibited • Cell loss in the hippocampus means reduced response to cortisol levels and loss of feedback inhibition of the HPA axis. • Antidepressant drugs reduce levels of CRF and reverse loss of hippocampal dendrites in animal studies • Cell loss in the hippocampus means reduced response to cortisol levels and loss of feedback inhibition of the HPA axis. • Antidepressant drugs reduce levels of CRF and reverse loss of hippocampal dendrites in animal studies. • .
Neurotrophic Hypothesis • Low BDNF (brain-derived neurotrophic factor) may be responsible for the loss of dendritic branches and spines in the hippocampus and PFC and for reduced neurogenesis in the hippocampus. • Antidepressants may prevent decrease of BDNF • Supporting evidence: • Chronic stress reduces BDNF in the hippocampus in rats. • Chronic but not acute antidepressant treatment increases BDNF in animals and humans. • Antidepressants prevent stress-induced reduction in BDNF and neuronal atrophy.
Neurotrophic Hypothesis Early life stress can lead to epigenetic changes that enhance CRF expression in the amygdala and hypothalamus and decreased glucocorticoid receptors in the hippocampus. The gene for BDNF can be modified by chromatin remodeling (epigenetic changes) that affect levels of gene expression.
Medical Chemical Electroconvulsive Shock Therapy Psychotherapy Cognitive Behavioral Therapy Interpersonal Therapy Depression: Treatment
Tricyclic Antidepressants • imipramine (Tofranil) • prevents monoamine reuptake • 64% respond well • many side effects • Monoamine Oxidase Inhibitors (MAOi) • phenelzine (Nardil) • blocks MAO enzyme • which breaks down monoamines • <64% respond well • several lethal side effects • Selective Serotonin Reuptake Inhibitors (SSRIs) • fluoxetine (Prozac) • blocks reuptake of serotonin • minor side effects Chemical Treatment
make patient examine thought process and recognize errors • arbitrary interference • overgeneralization • try to correct cognitive errors • concentrate on less depressive thoughts - be more realistic • target negative cognitive schemes • use journals to identify faulty thinking • do hypothesis testing • put fun back into the patients life • increase exercise • takes about 10-20 sessions Cognitive Behavioral Therapy