Download
1 / 15
150 likes | 375 Views
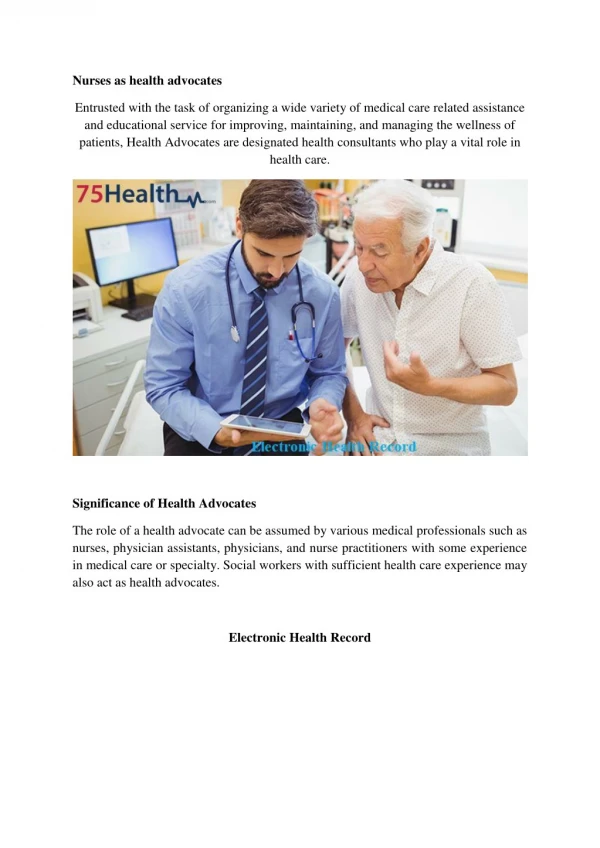
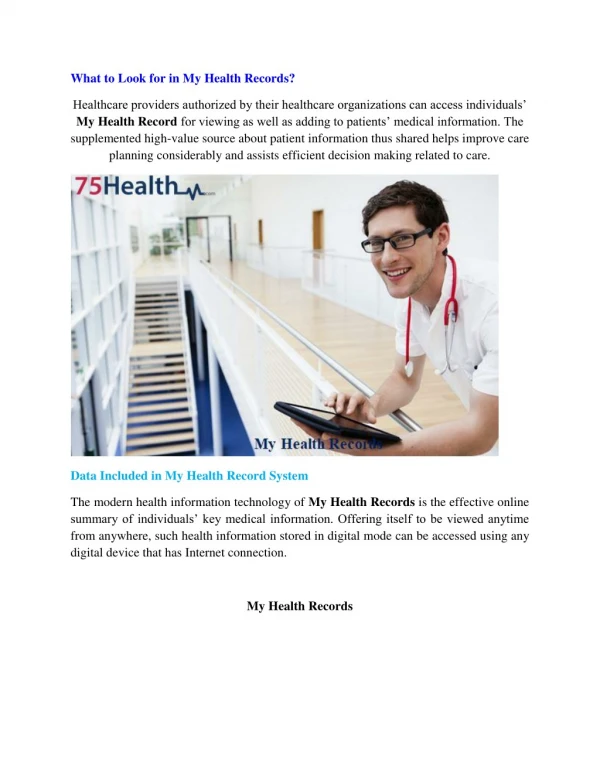
Introduction to the Electronic Health record. Chapter 1. Objectives. Brief understanding of the history of electronic health records Learn about the development and functionality challenges associated with creating electronic health records Develop a familiarity with meaningful use objectives.

E N D
Objectives • Brief understanding of the history of electronic health records • Learn about the development and functionality challenges associated with creating electronic health records • Develop a familiarity with meaningful use objectives
Key Concepts • Electronic health record • Closed system • Certification Commission for Health Information Technology • Health Information Technology for Economic and Clinical Health Act • Meaningful use • American Recovery and Reinvestment Act • Authorized testing and certification bodies
History • 1960s –first form of EHR • Developed by: Lockheed/Technicon for a hospital in California • Early systems evolved from another health care information technology system • Some were added to the front end of billing systems • Others were modified versions of a lab or imaging system • Many early EHRs solved only part of physician's needs for patient’s health care information due to complexity and variety of health care data needed
Closed System • Most EHR systems are closed-system • Data structures and programming code are proprietary to the company that developed them • Information is privately held by inventors and considered their intellectual property • This approach leads to lack of health care data exchange(interoperability) • Systems do not connect making it difficult near impossible for physicians to share clinical information
Certification Commission for Health Information Technology-CCHIT • Reviews and certifies the functionality of EHR systems • Developed standard definition of what an EHR should contain • Rates the usability of an EHR • Developed in response to the hundreds of choices on the market • CCHIT now recognized by the federal government as a certifying body • First organization of its kind
Health Information Technology for Economic and Clinical Health-HITECH • Healthcare political leaders recognized importance for our nation to have improved health care and pushed hard for legal solutions • 2009-U.S. federal government passed HITECH • Requires physicians to use an electronic health record system in order to treat patients whose care is paid by Medicare or Medicaid • Government to help pay for some of the costs over a five-year period • As long as physicians are using the certified EHR solutions they can get reimbursement from federal government by providing required documentation • If eligible physicians can receive as much as $44,000 over five years from Medicare or 63,750 over six years from Medicaid. • Hospitals may receive millions
Meaningful use • Set of health care quality measures that physicians need to capture using a certified EHR system. • Measures vary by patient volume and visit type • Using a certified EHR helps physicians to improve patient care, which will improve overall health of our nations population
Improving patient/nation health care • Improving Patient Care: Accurate, complete information about a patients health in order to give best possible care in routine or emergency situation. Ability to better coordinate care they give. Share information securely with patients, family caregivers over Internet, for those that would like this option. Patients can take more of a part in their health care. Information to help physicians diagnose health problems sooner, reduce medical errors and provide safer care at lower cost. • Improving the Nation’s Health: Can make our health care system more efficient, reduce paperwork for patients and physicians, expand access to affordable health care, and build a healthier future for our nation.
American Recovery and reinvestment act-ARRA • The office of the National Coordinator for Health Information Technology set up a process to approve companies as Authorized Testing and Certification Bodies (ATCBs) • Review EHRs based on a set of testing criteria for each of the core and menu measures.
Meaningful use objectives for ambulatory care • Centers for Medicare & Medicaid Services (CMS) describes qualifications for incentive payments for meaningful use; • EP (eligible professional)Physician must participate in Medicare and Medicaid EHR Incentives Programs • 20 of 25 objective must be met • All 15 core objective for ambulatory meaningful use must be met • Five of menu objectives for ambulatory meaningful use must be met
Core Objectives for ambulatory meaningful use • Use Computerized Provider Order Entry (CPOE) • Implement Drug/Allergy Interaction Checking • Maintain Problem List • Generate ePrescriptions • Maintain Active Medication List • Maintain Active Medication Allergy List • Record Demographics • Record Vital Signs • Record Smoking status • Report Ambulatory Quality Measures • Implement Clinical Decision Support
Cont.…Core Objectives for ambulatory • 12. Provide patients with EHR Copy • 13. Provide Clinical Summaries • 14. Exchange Key Clinical Information • 15. Protect Electronic Health Information
Menu objectives for ambulatory meaningful use • Drug Formulary Checks • Clinical Lab Test Results • Patient Lists • Patient Reminders • Timely Access • Patient-Specific Education Resources • Medication Reconciliation • Summary Care Record • Immunizations Registries • Syndromic Surveillance Data
Exclusions • Certain objectives provide exclusions. • If an EP meets the criteria for exclusions, then EP can claim that exclusions during attestation • If exclusions is not provided, of if EP does not meet the criteria for an existing exclusion, then the EP must meet the measure of the objective in order to successfully demonstrate meaningful use and receive an EHR incentive payment • Failure to meet the measure of an objective or to qualify for exclusion for the objective will prevent the EP from successfully demonstrating meaningful use and receiving an incentive payment • Hospital core and menu objectives apply to inpatient settings which are not covered in this textbook. Hospitals have additional objectives that the ambulatory setting does not